Download to read offline
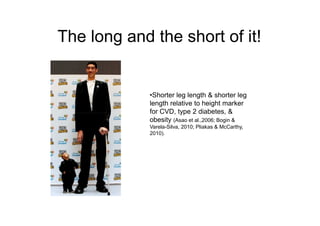



This document summarizes the development and validation of a new field-based tool for measuring body proportionality among children. It was created by Jabeen Shah for a postgraduate research conference. The tool aims to provide a lightweight, portable, and inexpensive alternative to current laboratory measures of sitting height and leg length ratios, which are markers of obesity, diabetes, and cardiovascular disease risk. Initial results found the adapted measure to have high validity and reliability compared to standard measures, with a low coefficient of variation, suggesting it is suitable for use in field studies.


































































