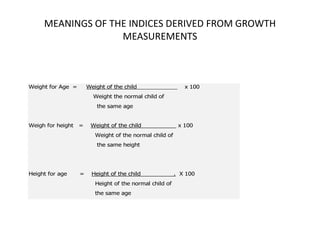
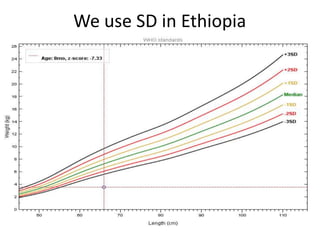
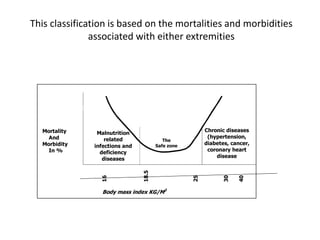
This document provides an overview of nutritional assessment methods. It discusses both direct and indirect assessment approaches. Direct methods include anthropometric, biochemical, clinical and dietary assessments. Anthropometric assessments measure the body and include indices like BMI, MUAC and skin fold thickness. Biochemical assessments involve laboratory tests. The document focuses on anthropometric methods and their purposes in assessing growth in children and body composition in adults. It provides details on specific anthropometric measurements and derived indices along with their clinical meanings and cut-off points.