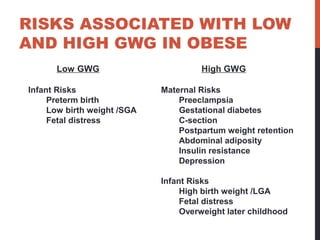
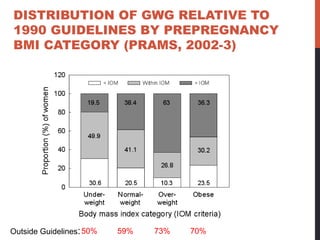
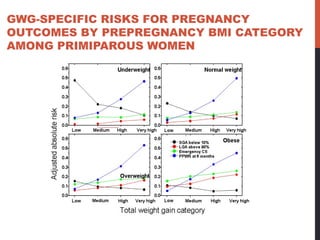
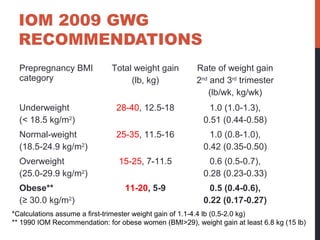
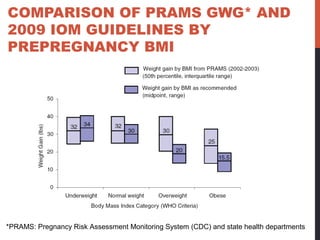
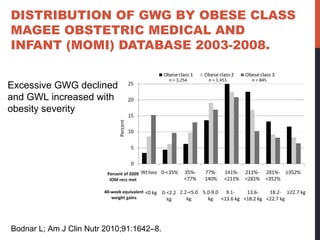
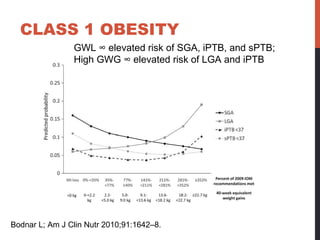
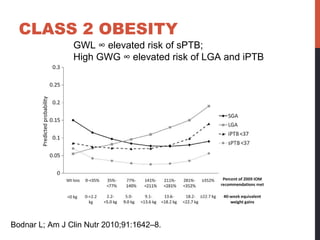
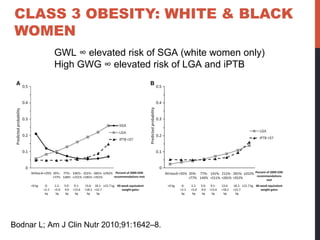
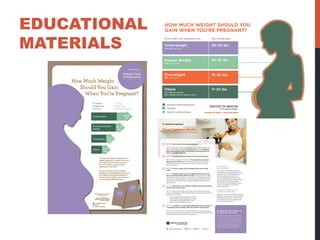
The document provides guidelines for gestational weight gain in obese pregnant women. It summarizes that the majority of obese women gain weight outside existing guidelines, and both low and high gestational weight gain are associated with risks for mother and child. The 2009 Institute of Medicine guidelines recommend a weight gain range of 5 to 9 kg for obese pregnant women, though data on optimal gain levels according to obesity severity are still limited. Some studies have found benefits of minimal or no weight gain for more severely obese women, though larger studies are still needed.