The document discusses iron deficiency anemia, including its definition, symptoms, causes, stages, diagnostic tests, and treatment options. Key points include:
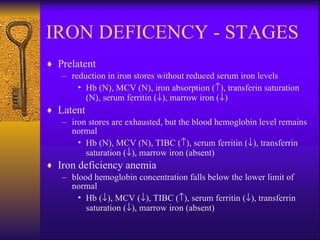
- Iron deficiency anemia is defined as a reduction in hemoglobin concentration below the reference value.
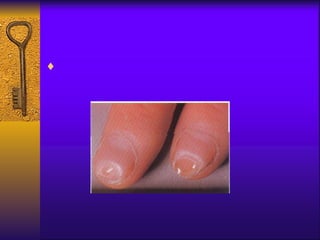
- Symptoms include fatigue, dizziness, and headaches. Specific symptoms like glossitis or koilonychia may also occur.
- Causes include chronic bleeding, decreased iron intake, and increased iron requirements during growth or pregnancy.
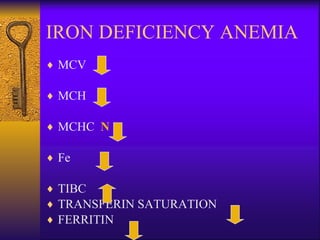
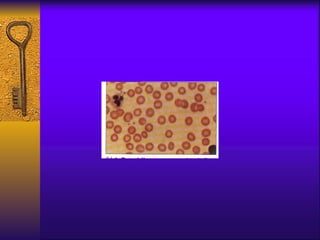
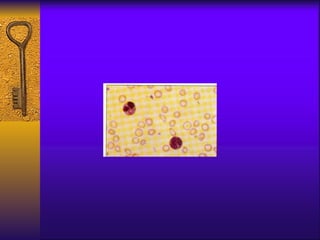
- Diagnosis involves blood tests measuring iron levels, iron binding capacity, ferritin, and a bone marrow smear.
- Treatment options include oral or parenteral iron supplementation to restore iron stores over 6-9





















































![Iron Deficiency Anemia [Autosaved] by SM.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/irondeficiencyanemiaautosaved-250701032035-c41a782a-thumbnail.jpg?width=640&height=640&fit=bounds)





































