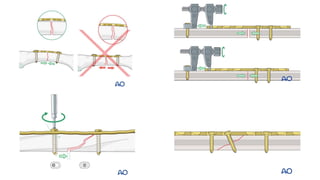
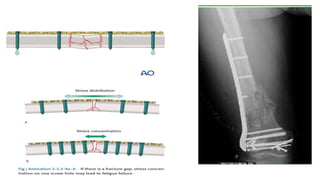
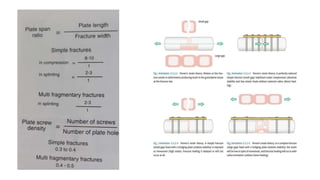
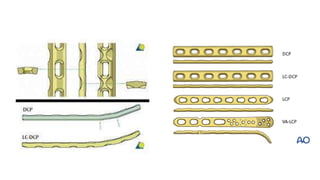
Bone plates are used to stabilize fractures and allow healing. There are several types of plates that serve different purposes: protection plates neutralize forces to protect fractures fixed with lag screws, compression plates apply tension to achieve compression at the fracture site, bridge plates span multifragmentary fractures without disturbing the fracture, and buttress/antiglide plates resist forces perpendicular to the axis of deformity. More recently, locking plates have been developed that use locked screws to provide stability without compressing the bone, reducing stress shielding and risk of infection compared to conventional plates.
![Classification/ Principles
• Protection [ neutralization] plate
• Compression plate
• Bridge plate
• Buttress plate
• Condylar plate
• Tension band plate](https://image.slidesharecdn.com/boneplates-220925130903-da2301d7/85/Bone-plates-3-320.jpg)
![Protection [ Neutralization ] Plate
• Plate is applied as an adjunct to lag screws.
• In fractures such as short oblique, butterfly fragments, etc,
interfragmentary compression is achieved by the lag screws and the
construct is further protected from bending , torsional and shearing
forces.
• Healing takes place via primary healing.](https://image.slidesharecdn.com/boneplates-220925130903-da2301d7/85/Bone-plates-4-320.jpg)
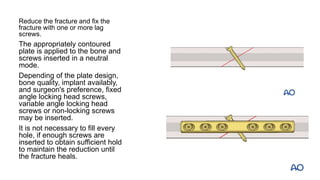


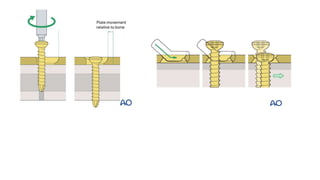


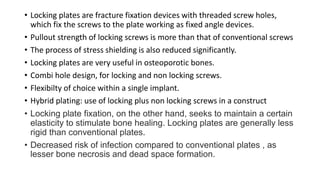
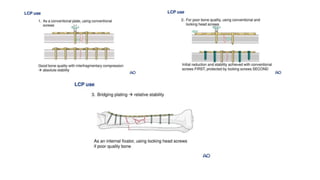
![Locking plates [ LCP ]
• Latest type of plate design or evolving technique of plating.
• It is used as a internal fixator.
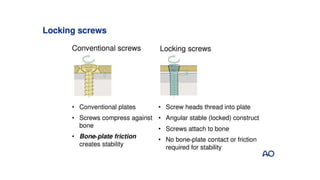
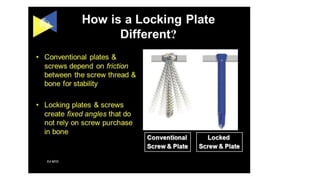
• The pitch of the screw head is identical to the pitch of the screw body to prevent
compression.
• There are fixed angle and variable angle plating systems available.
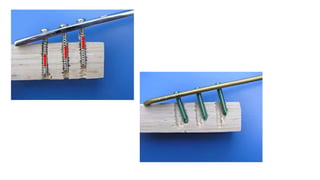
• Shearing forces are better tolerated as compared to conventional screws and
resistance to pullout is high.
• Extraperiosteal placement, thus maintaining the periosteal blood supply by
reducing the bone plate interface.
• As the screws are tightened, they "lock" to the plate, thus stabilizing the
segments without the need to compress the bone to the plate.
• advantage to the use of locking plate/screw systems is that the screws are
unlikely to loosen from the plate.](https://image.slidesharecdn.com/boneplates-220925130903-da2301d7/85/Bone-plates-31-320.jpg)