This document provides information on intensifying screens and radiographic grids. It discusses the history, construction, and functions of intensifying screens, including the types of phosphors used. It also covers screen speed, detail, and care. For radiographic grids, it outlines the history and development of grids as well as grid design, patterns, specifications and factors such as ratio and frequency. Research studies evaluating different screen-film combinations and their effects on image quality and radiation dose are also summarized.

![Currently, there are two groups of X-ray films for dental purposes:
1. Non-screen - Those with emulsions more sensitive to direct exposure of
X - rays.
These are primarily used as intraoral films and provide excellent image
quality.
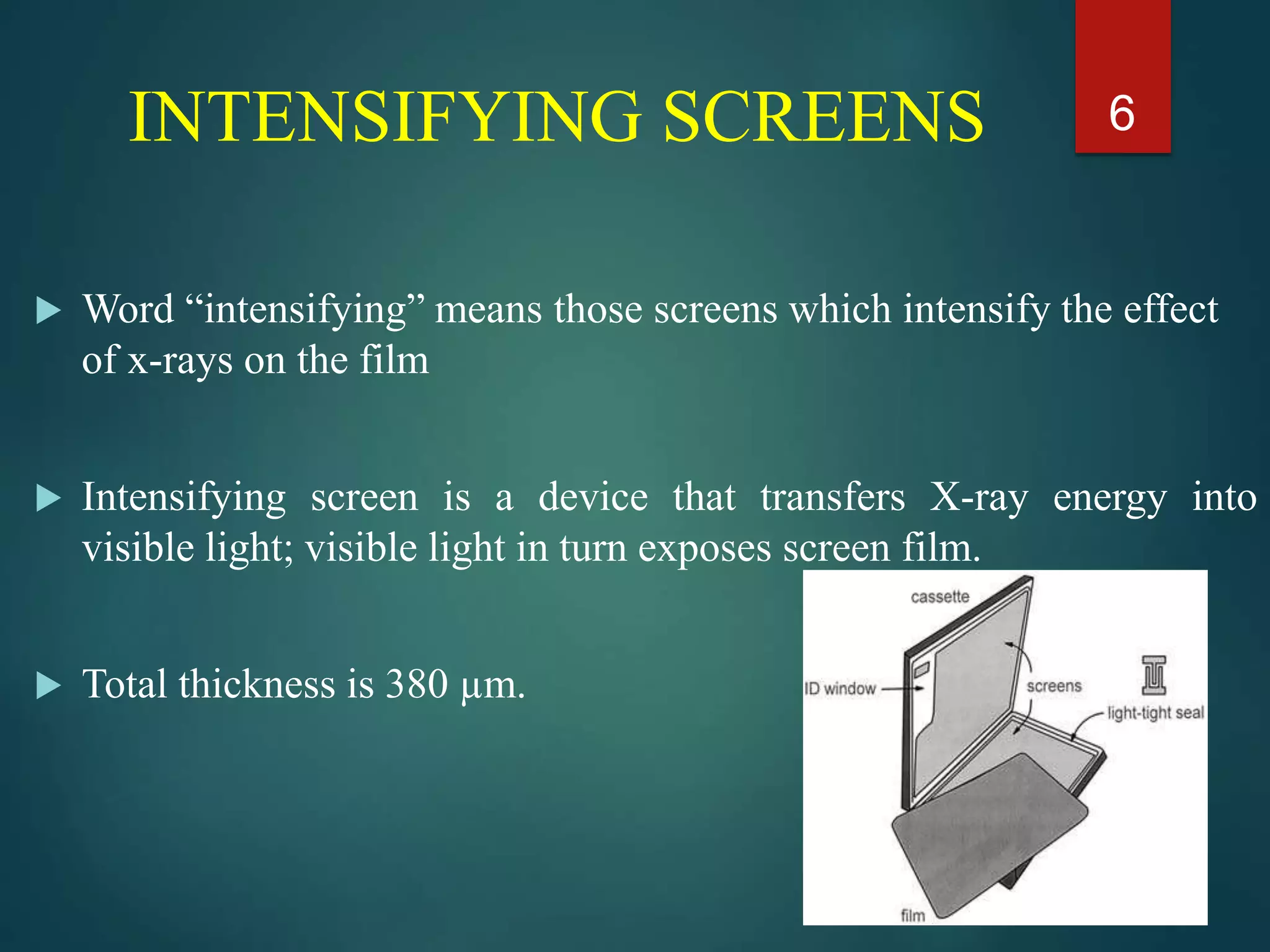
2. Screen - Those with emulsions more sensitive to blue [standard] OR green
[rareearth] light.
Emitted when X-rays strike the intensifying screens.
The X-ray photons are converted to visible light photons.](https://image.slidesharecdn.com/intensifyingscreensandgrids-230522090944-e7f15b88/75/intensifying-screens-and-grids-pptx-5-2048.jpg)