Downloaded 37 times













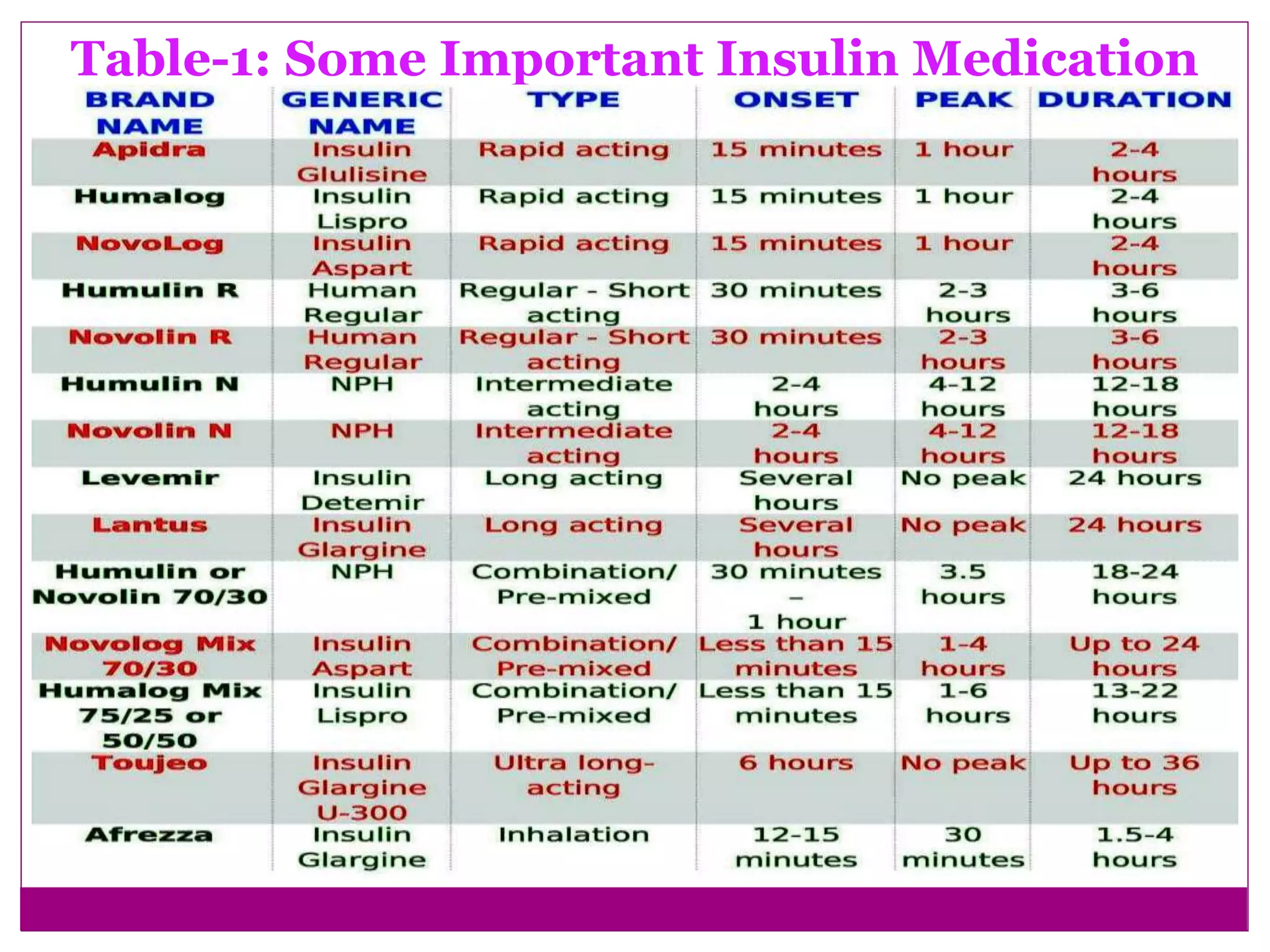


























The document provides a comprehensive overview of insulin, detailing its structure, function, and significance in regulating blood sugar levels, as well as the historical journey of its discovery and development. It discusses different types of insulin medications, their characteristics, adverse effects, and dosing considerations for individuals with diabetes. Additionally, it outlines safe storage practices and the impact of various conditions on insulin therapy.
















































































