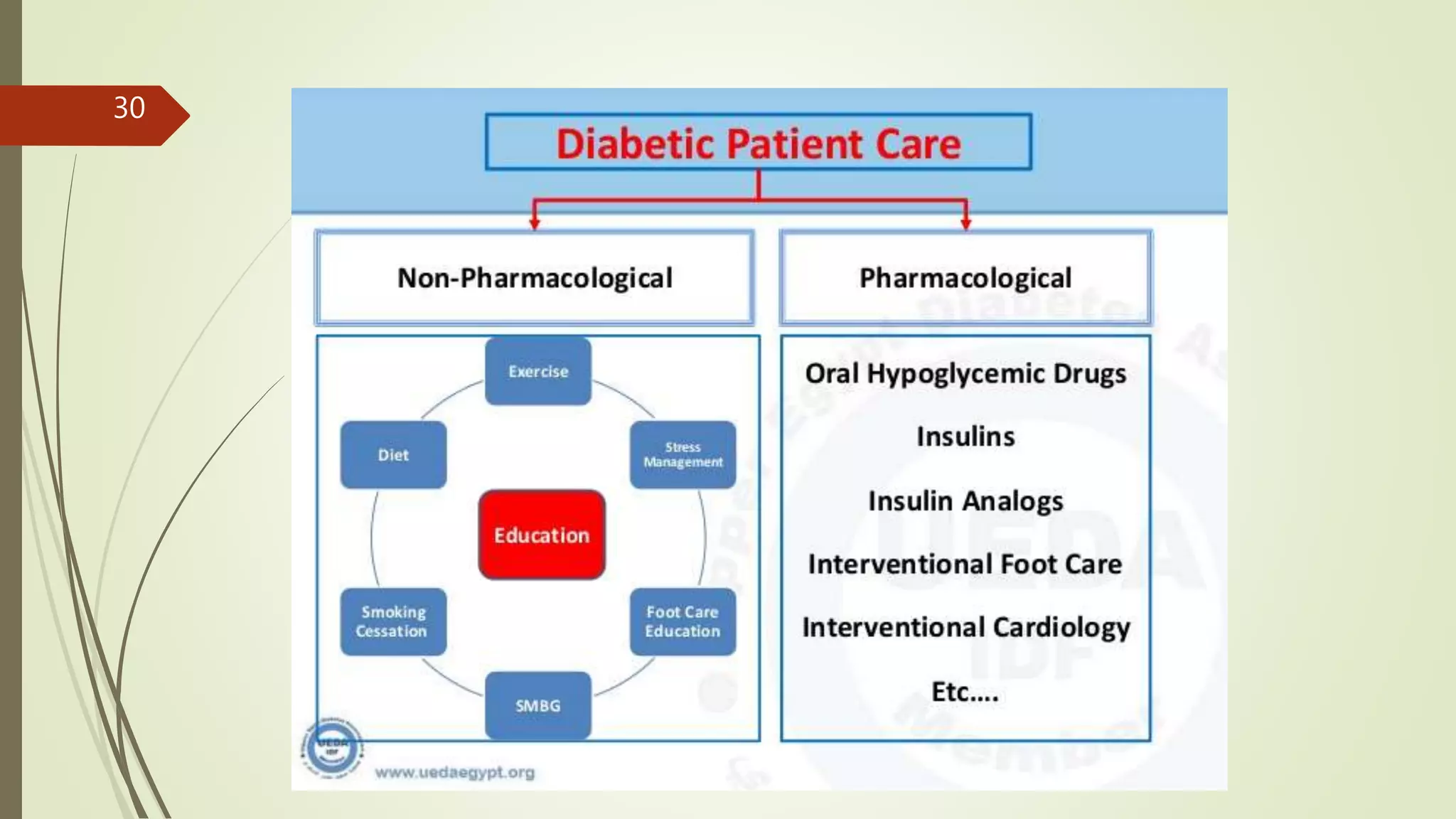
Diabetes is a heterogeneous group of syndromes characterized by elevated blood glucose due to insulin deficiency. Its prevalence has markedly increased, with significant historical context tracing back to ancient civilizations. The document discusses the pathogenesis, classification, diagnosis, and various management strategies for diabetes, emphasizing the importance of prevention and self-care.







































































































































![DM lecture for c1 [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/dmlectureforc1autosaved-220720190831-86418752-thumbnail.jpg?width=640&height=640&fit=bounds)





















