Downloaded 31 times


- Type 2 diabetes accounts for over 90% of diabetes cases worldwide and is associated with obesity, lack of exercise, and poor diet. It is managed through lifestyle modifications including diet, exercise, oral hypoglycemic medications, and sometimes insulin therapy. - The main treatment approaches involve dietary changes to control blood sugar and weight, regular physical activity, oral medications like metformin and sulfonylureas, and potentially insulin therapy if blood sugar levels remain uncontrolled. - Close monitoring of blood sugar levels through self-testing and HbA1c levels helps guide treatment adjustments and ensure proper management of the disease.
Introduces diabetes management, outlines key topics: definition, epidemiology, classification, clinical features, and treatment.
Defines diabetes mellitus as a chronic metabolic disorder caused by insulin deficiency leading to hyperglycemia.
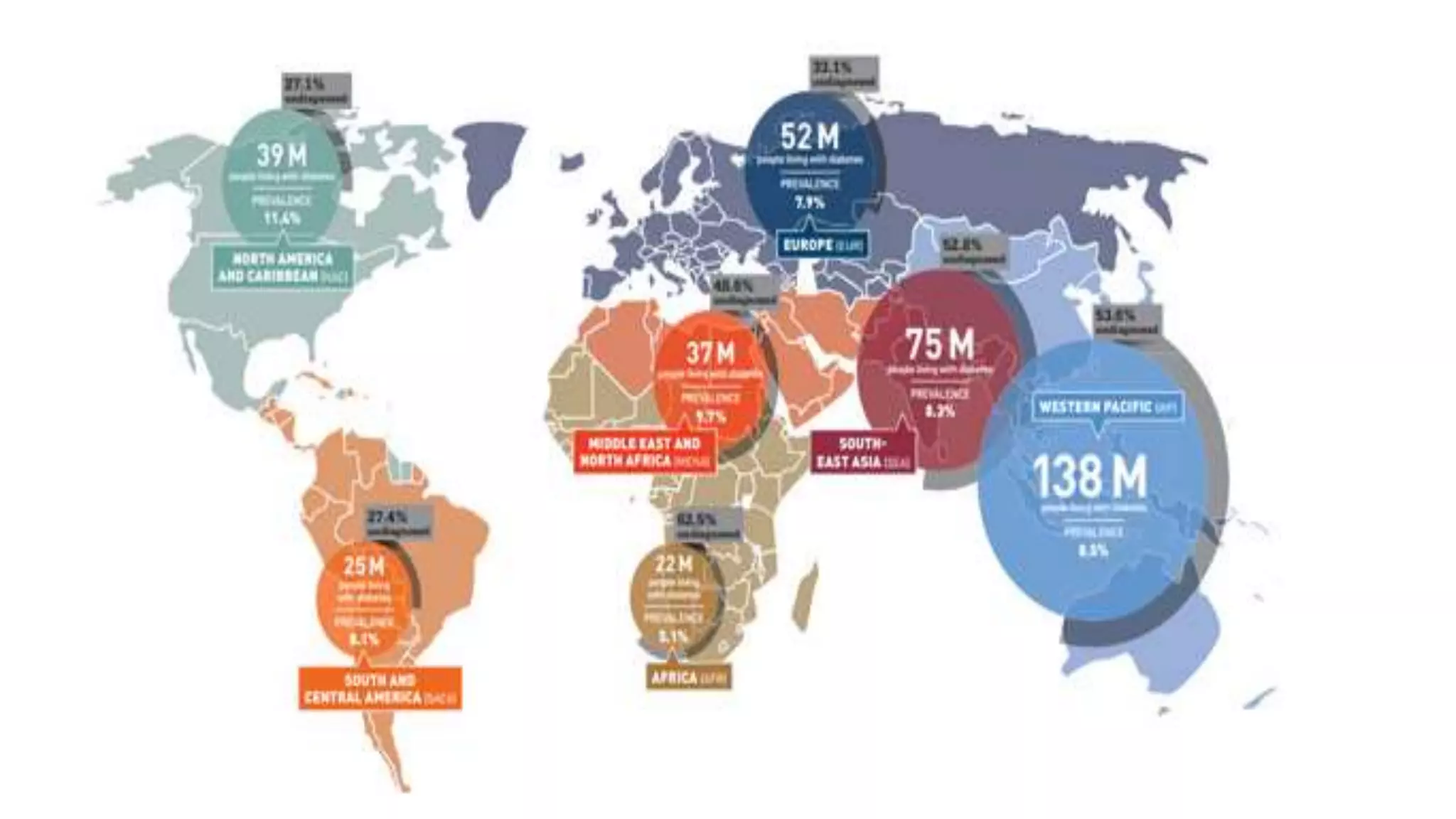
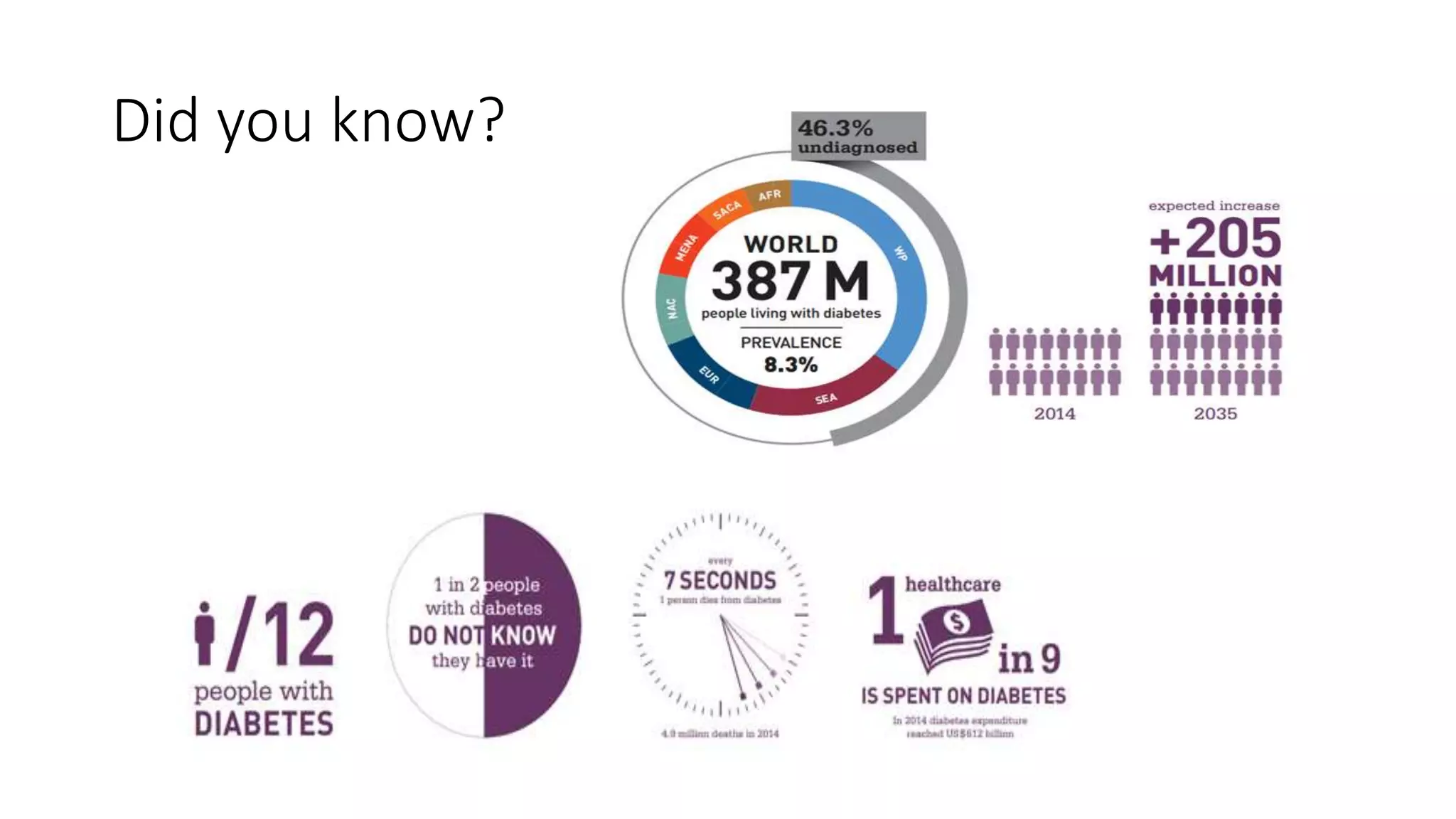
Highlights global diabetes statistics: >380 million globally, 1.56 million in Uganda (2014), 4.4% prevalence, and a significant undiagnosed population.
Classifies diabetes into: Type 1, Type 2, Gestational diabetes, and diabetes due to other causes.
Discusses Type 1 diabetes: diagnosis in childhood, autoimmune factors, environmental influences, and LADA.
Describes Type 2 diabetes: common in adults, links to obesity and lifestyle, with childhood cases rising.
Describes gestational diabetes, its risk factors, prevalence in pregnancies, and potential progression to Type 2 diabetes.
Lists symptoms of diabetes: polyuria, weight loss, fatigue, dehydration, complications like retinopathy and neuropathy.
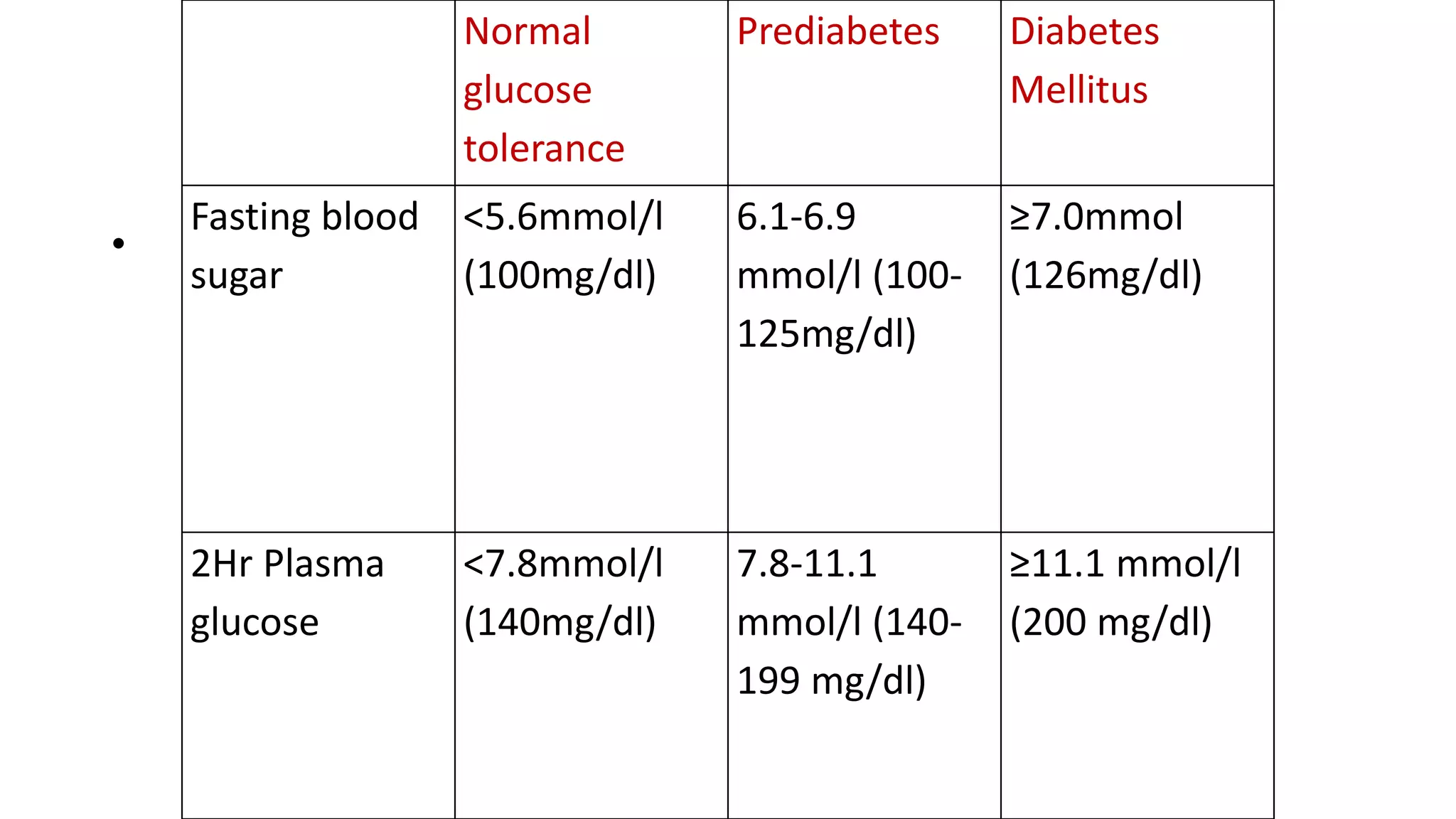
Outlines diagnostic criteria for diabetes including blood sugar levels and testing methods like OGTT.
Discusses the approach to managing diabetes through thorough history taking and physical examination.
Lists investigations needed for diabetes management: urinalysis, blood glucose testing, and lipid profile.
Details treatment components: Diet, Exercise, Oral hypoglycemics, and Insulin therapy.
Emphasizes correct diagnosis, self-care, teamwork, and controlling cardiovascular risk factors.
Details dietary management focusing on nutrient balance, caloric intake, and glycemic control.
Discusses exercise benefits for weight reduction and improved insulin sensitivity.
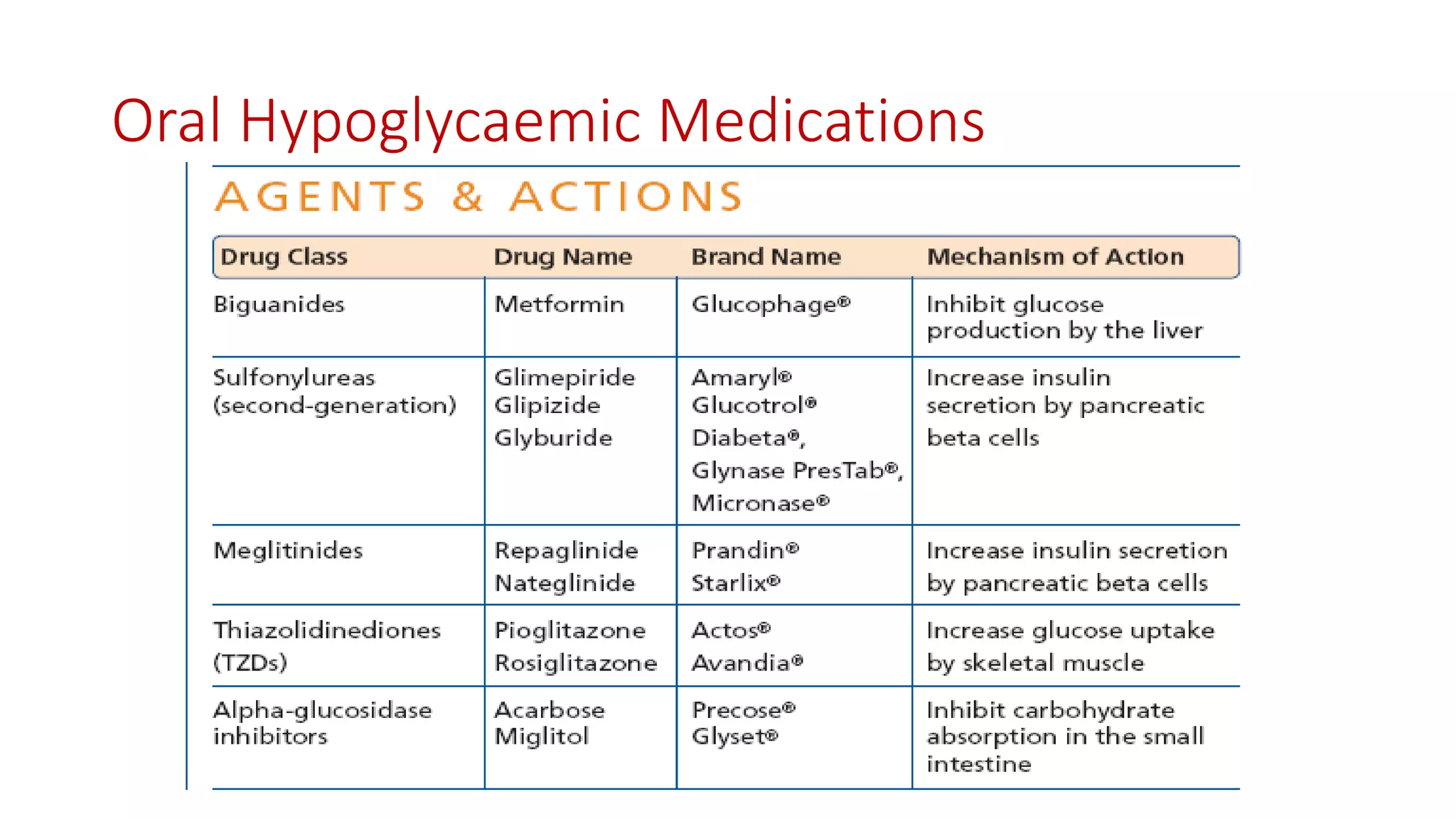
Describes oral agents for diabetes management, categorization, and their application in treatment phases.
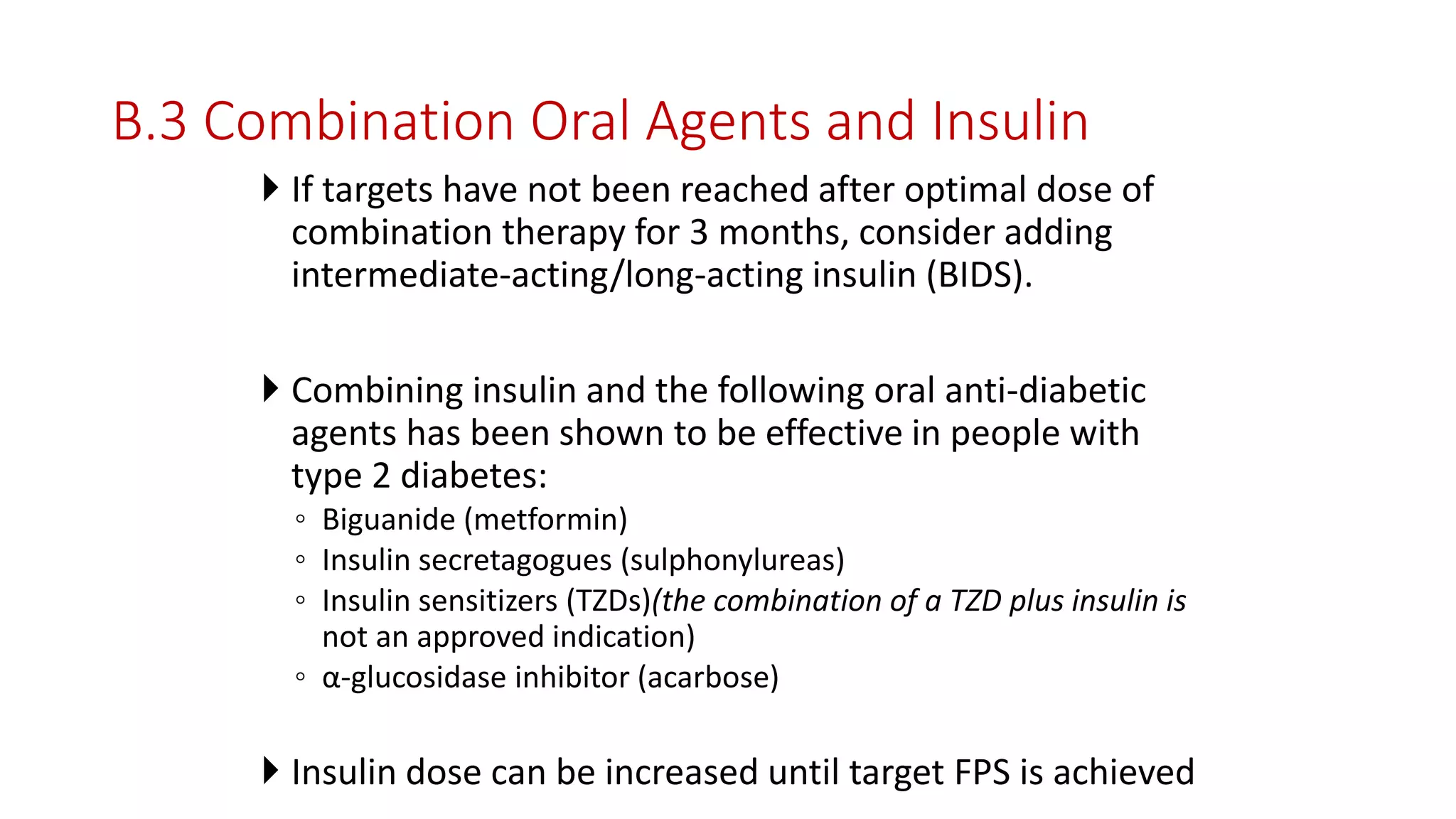
Details the combination therapy of insulin with oral anti-diabetic agents for improved glycemic control.
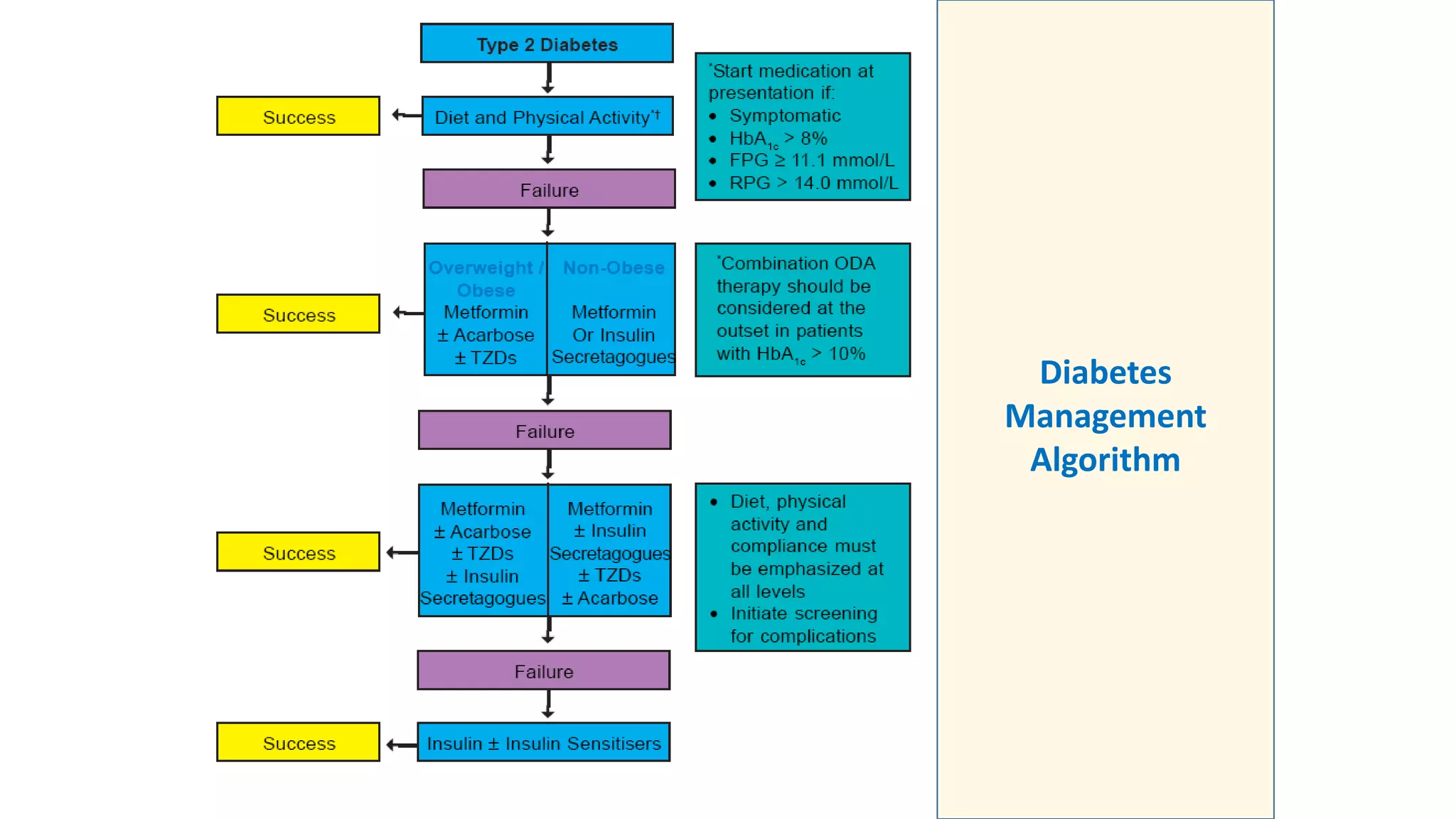
Presents a visual representation of diabetes management strategies.
Offers guidelines for oral medication use in diabetes, especially in special cases like pregnancy.
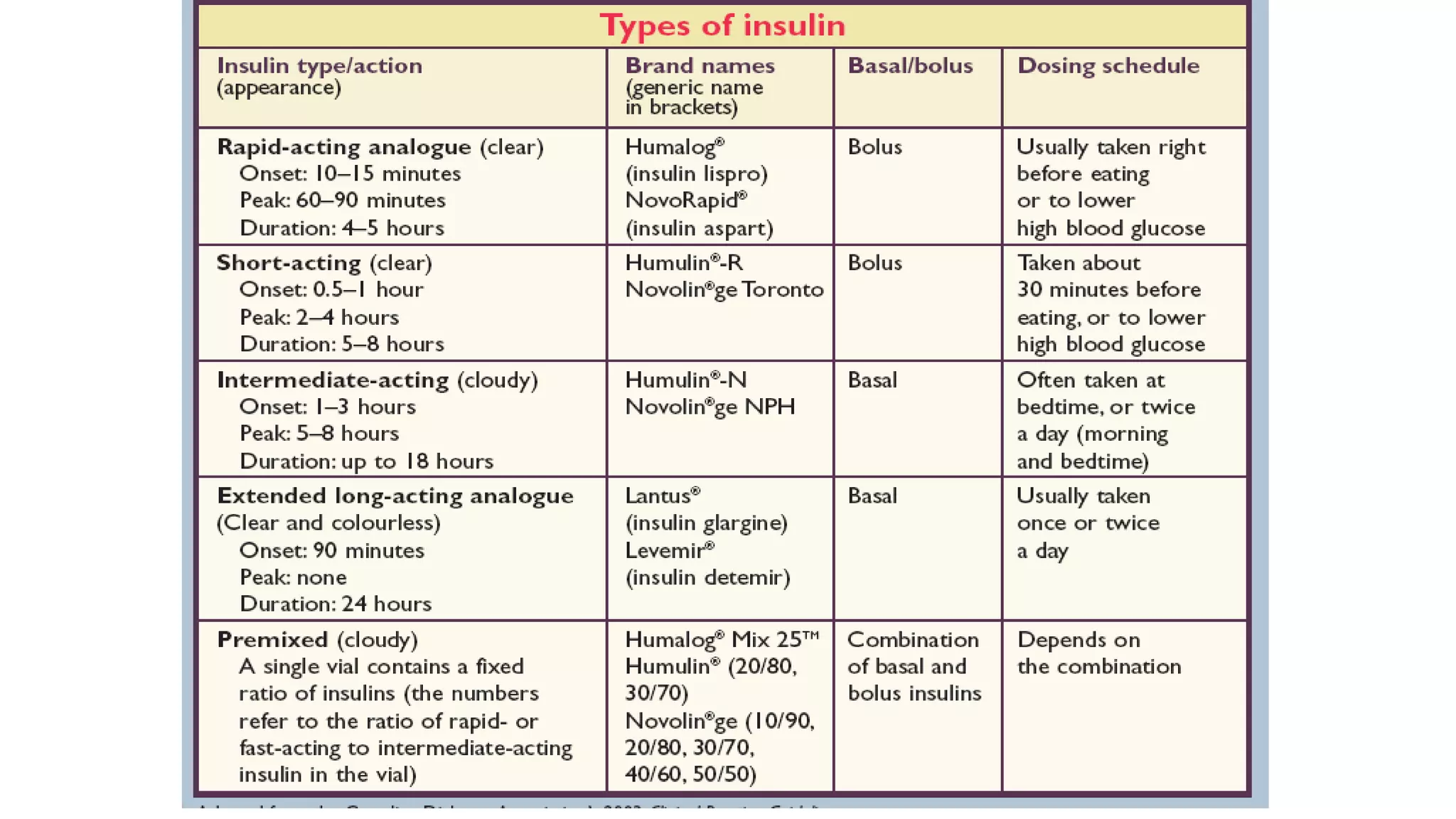
Discusses when to initiate insulin therapy, types of regimens, and insulin use in treatment.
Emphasizes self-monitoring practices and how to assess glycemic control through HbA1C measurements.
Highlights the need for patient education in self-management practices to take control of diabetes.
Thanks attendees and concludes the presentation.




























































































