Downloaded 1,866 times


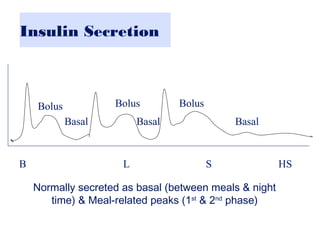
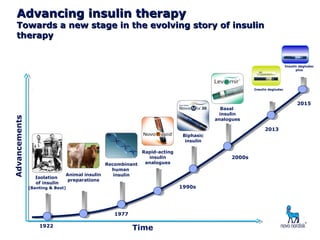
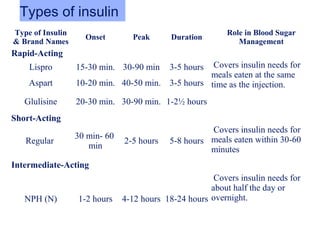
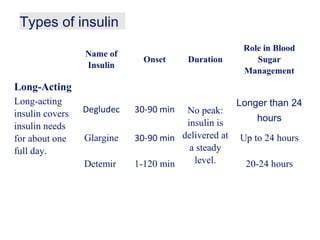
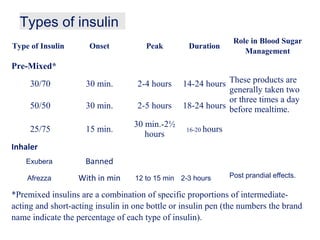
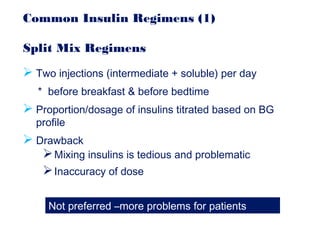

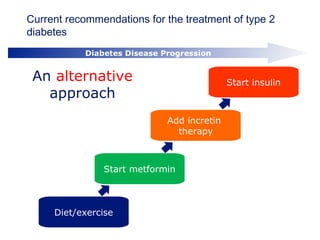



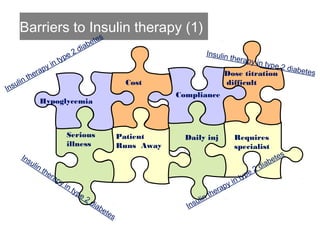
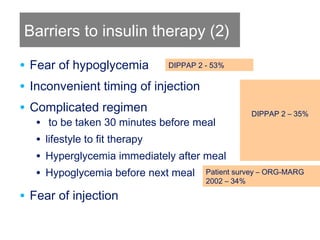



This document provides information on insulin therapy. It discusses what insulin is, how it is secreted normally, and its actions in the body. Insulin deficiency results in hyperglycemia and other metabolic defects. The discovery of insulin by Banting and Best in 1921 revolutionized the treatment of diabetes. Insulin comes in various forms including rapid-acting, short-acting, intermediate-acting, long-acting, and premixed varieties. Common insulin regimens include split-mixed, basal, basal-plus, and basal-bolus. Early initiation of insulin in type 2 diabetes has clinical benefits beyond glycemic control. Barriers to insulin therapy include fear of hypoglycemia and the inconvenience of injection schedules. Pro