Downloaded 13 times













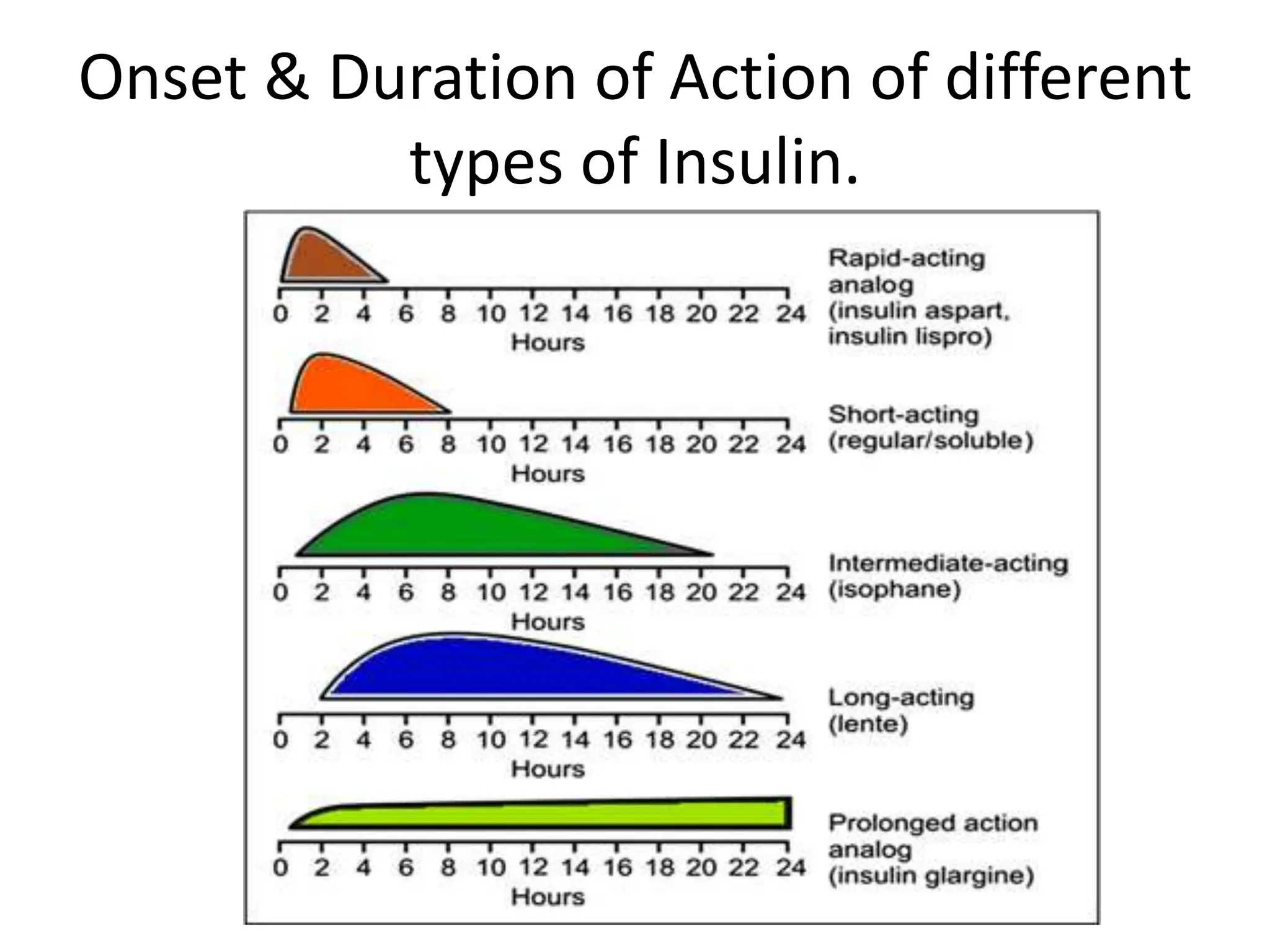





























There are several types of insulin that differ in their onset of action, peak time, and duration. Rapid-acting insulin starts working within 15 minutes and has a duration of 3-4 hours. Regular or short-acting insulin starts within 30 minutes and lasts 6 hours. Intermediate-acting insulin starts within 2-4 hours and lasts 12 hours. Long-acting insulin starts within 2-4 hours and lasts up to 24 hours. Premixed insulin starts working within 15-30 minutes and lasts 12-16 hours. Inhaled insulin starts within 10 minutes and lasts 3 hours. The document also discusses the properties and uses of different insulin analogs and human insulins.










































![diabetes.pptxgtgthtgtgtgthyjiulp'][pp0ppp](https://cdn.slidesharecdn.com/ss_thumbnails/diabetes-250824142109-beeb6b11-thumbnail.jpg?width=640&height=640&fit=bounds)












































