Downloaded 728 times













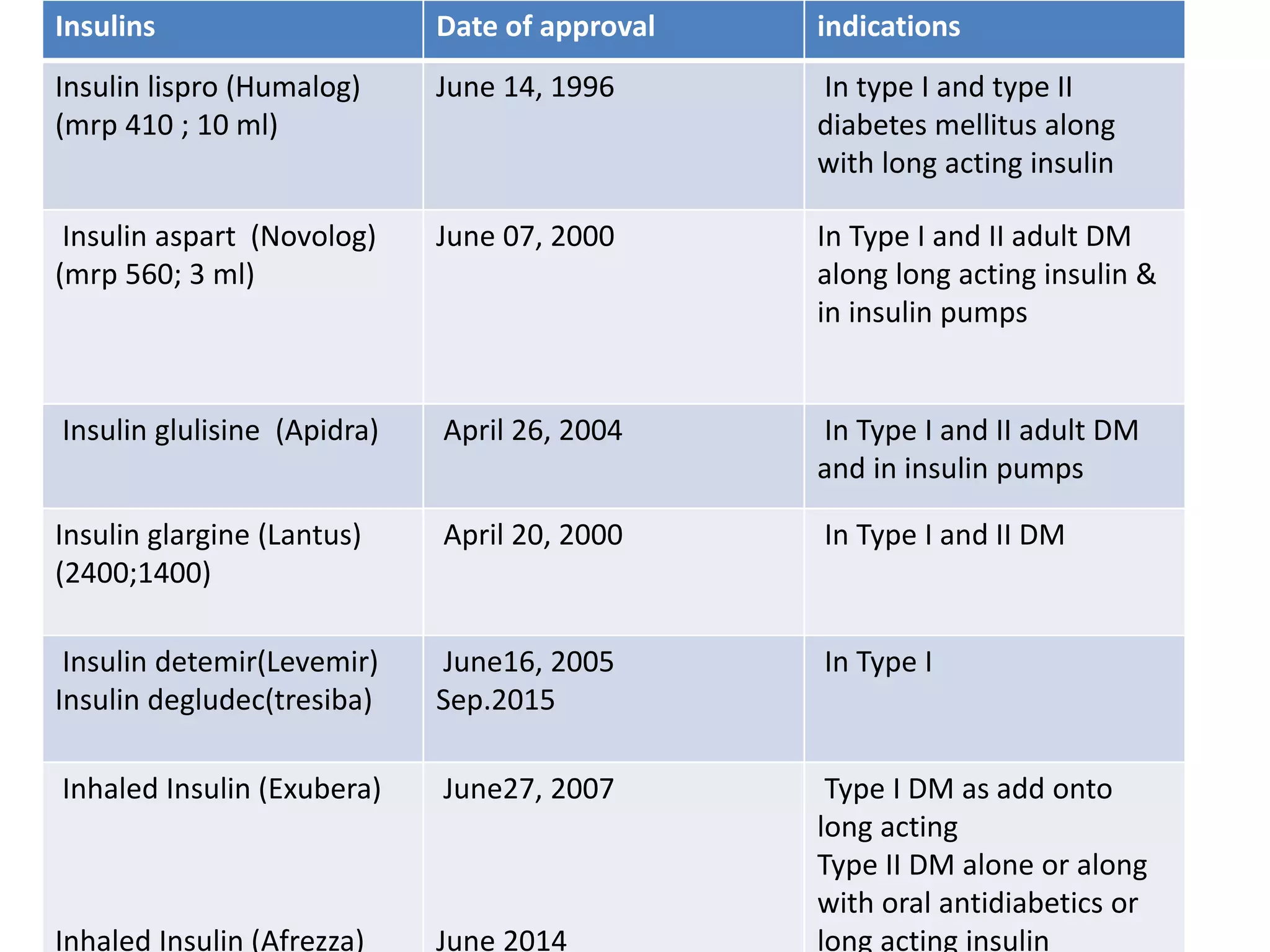























































The document summarizes different types of insulin, including human insulin and newer insulin analogues. It describes the structure and production of human insulin and discusses problems with conventional insulins like regular insulin. It then provides details on various short-acting and long-acting insulin analogues like insulin lispro, insulin glargine, insulin detemir, and insulin degludec, including their structures, mechanisms of action, advantages over human insulin, dosing, and pregnancy categories. The document also briefly mentions other newer insulins under development or approval like inhaled insulin and insulin fusion proteins.












































































