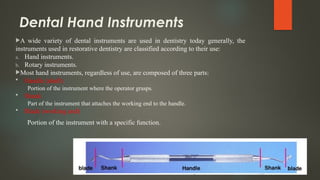
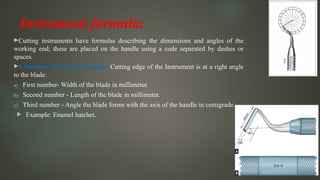
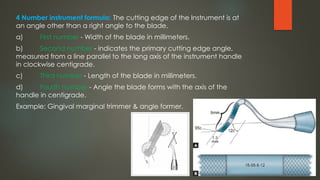
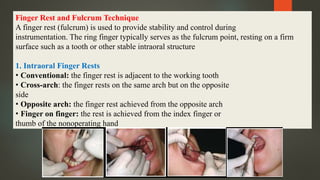
This document provides a comprehensive overview of dental hand instruments used in cavity preparation, categorizing them into hand, rotary, and ultrasonic instruments, and detailing their specific functions and uses. It explains instrument classification, formulas for cutting instruments, and various hand and rotary instrument types, alongside their operational techniques and operator positioning. The text emphasizes the anatomy of instruments, methods of instrument grasping, and techniques for patient and operator positioning during dental procedures.



























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















