Downloaded 63 times
































![INDICATORS OF POOR PROGNOSIS FOR TWIN
REVERSED ARTERIAL PERFUSION (TRAP SEQUENCE)
• Ratio of weight of the acardiac twin/weight of the pump twin greater than 0.70.
• weight (grams) = (-1.66 x longest length[cm]) + (1.21 x longest length[cm])
• Polyhydramnios (maximum vertical pocket ≥8 cm)
• Cardiac failure in the pump twin may be marked by abnormal Doppler studies including persistent
absent or reversed diastolic blood flow in the umbilical artery, pulsatile blood flow in the umbilical
vein, and/or reversed blood flow in the ductus venosus.
Ratio of Acardiac twin to the pump twin Risk of preterm delivery (%) Risk of polyhydramnios (%)
>0.70 90 40
<0.70 75 30
Moore, Thomas R. et al. Perinatal outcome of forty-nine pregnancies complicated by acardiac
twinning American Journal of Obstetrics & Gynecology , Volume 163 , Issue 3 , 907 - 912](https://image.slidesharecdn.com/twinsutz-190928095059/85/Twins-utz-42-320.jpg)














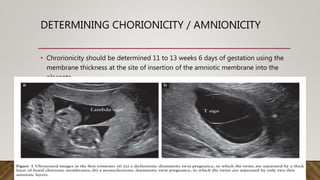
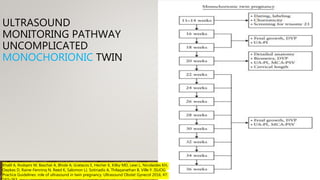
Ultrasound plays an important role in managing twin pregnancies by determining chorionicity, labeling and monitoring fetuses, screening for abnormalities, assessing growth and well-being, and detecting complications. Routine scans are recommended every 4 weeks for uncomplicated dichorionic twins and every 2 weeks for monochorionic twins. Additional monitoring may be needed based on conditions like selective fetal growth restriction. Management of complications is best done at tertiary centers.























































































