Downloaded 37 times
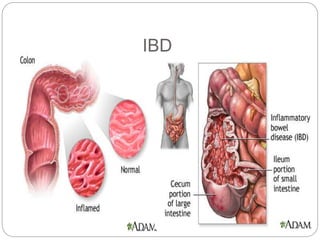
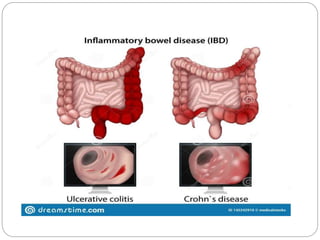
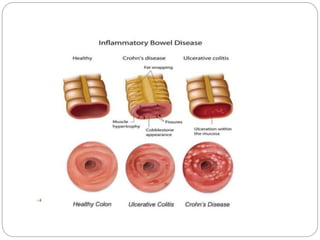
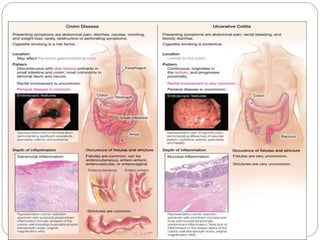
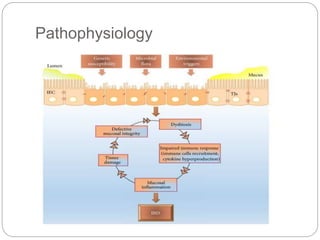

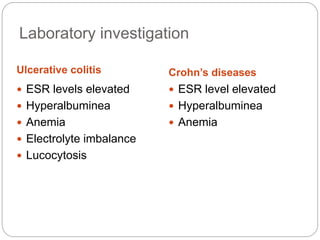
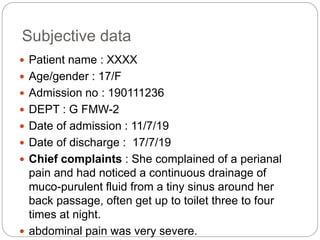
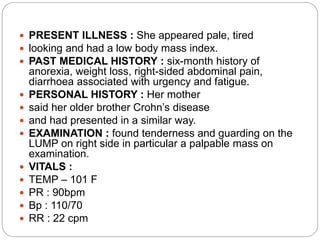
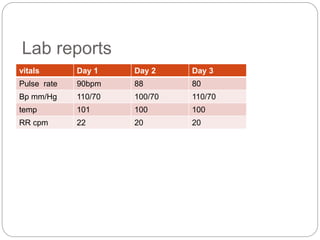
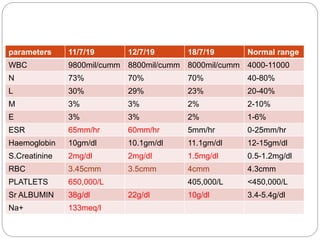
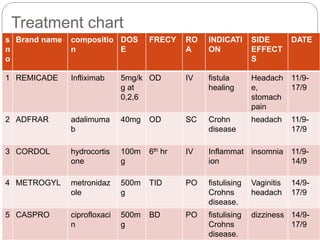
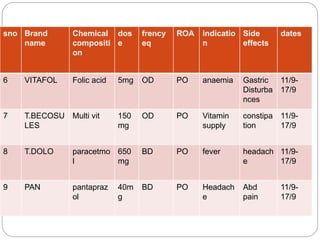
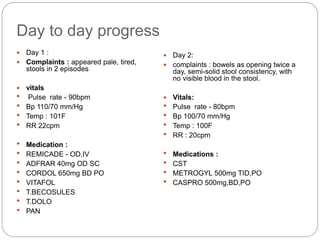
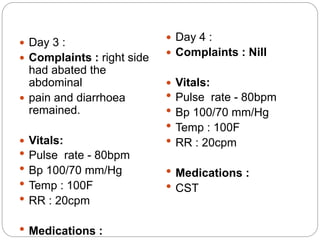
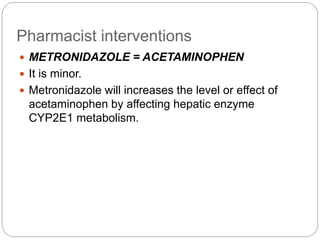
This document presents a case study on inflammatory bowel diseases. It provides definitions and classifications of inflammatory bowel diseases, specifically ulcerative colitis and Crohn's disease. It describes the symptoms, risk factors, laboratory findings, investigations, assessments, treatment and lifestyle modifications for a 17-year-old female patient admitted with complaints of perianal pain and drainage who was diagnosed with Crohn's disease. Her symptoms improved with medical treatment including infliximab and she was discharged on a low residue diet and continuing medications.










































































