Inflammatory Bowel Disease
Presenter: Dr. Sujan Khadka(2nd
year)
Moderator :Dr. Sushil Subedi
Date :2081/01/23
Pokhara Academy of Health Sciences
2.
Table of Contents:
Introduction
Types
Aetiologyand pathology
Distinguishing features of ulcerative colitis and Chron’s disease
Principles of medical management
Role of surgery in acute and elective settings
Management of post operative complications
Long term outcomes
3.
Definition and Types:
Theterm Inflammatory Bowel Disease (IBD) refers to a
conditions characterized by presence of idiopathic intestinal
inflammation.
Types:
• Crohn disease (CD)
• Ulcerative colitis (UC)
4.
Epidemiology
The incidence andprevalence of IBD is highest in Europe and North
America
Affects around 3 in 1000 people.
Overall incidence is steadily increasing worldwide
Linked to improved public hygiene, dietary changes, and
industrialization.
5.
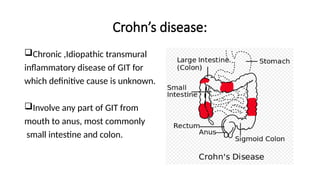
Crohn’s disease:
Chronic ,Idiopathictransmural
inflammatory disease of GIT for
which definitive cause is unknown.
Involve any part of GIT from
mouth to anus, most commonly
small intestine and colon.
6.
Crohn’s disease:
History:
• 1st
documentedcase described by Morgagni in 1761
• 1913 Scottish surgeon Dalziel described 9 cases of intestinal
inflammatory disease
• 1932,Landmark paper by Crohn and collogues provided the
pathologic and clinical findings of this inflammatory disease in young
adults.
Incidence: Male and female affected equally.
Distribution: Bimodal
7.
Crohn’s disease:
Risk factors:
•Family history: First degree relatives with Crohn's disease
• Smoking(twice than non smokers)
• Drugs:(oral contraceptives, Aspirin, NSAIDs)
• Diet: Decrease dietary fibres , increase fat intake
• Ethnicity: Ashkenazi Jews has 2-4 fold higher incidence.
Pathophysiology:
Mutations of theNOD2 gene → defects in the lamina propria and
epithelial barrier of the gastrointestinal (GI) tract → more pathogens
penetrate the GI tract → recruitment and activation of cytotoxic cells.
Activation of Th1-mediated cells in the GI wall → release of pro-
inflammatory cytokines(like IL-2 and TNF) → intestinal inflammation.
Lack of the down-regulation of immune responsiveness after an
infection or initial flare → chronic inflammation → granulomas
10.
Pathophysiology:
Intestinal tissue damageincluding edema, ulcerations, erosions and
necrosis
Since the inflammation is transmural, it may lead to intestinal
perforation and fistulas.
Chronic and repetitive episodes → scarring
Fibrosis and obstruction of the intestinal wall.
11.
Crohn’s disease:
Pathology:
• Mayinclude any portion of the GI tract.
• The most common site is terminal ileum and proximal colon.
• Associated with skip lesions
• The rectum is often spared.
12.
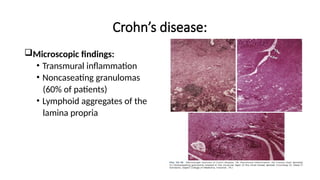
Crohn’s disease:
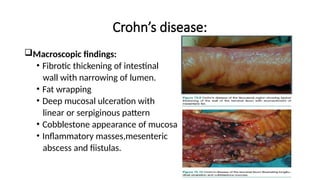
Macroscopic findings:
•Fibrotic thickening of intestinal
wall with narrowing of lumen.
• Fat wrapping
• Deep mucosal ulceration with
linear or serpiginous pattern
• Cobblestone appearance of mucosa
• Inflammatory masses,mesenteric
abscess and fiistulas.
Clinical features:
Symptoms:
• GImanifestations:
Chronic, intermittent diarrhea that is usually non-bloody.
Intermittent and colicky abdominal pain (may be diffuse or localized
to the right lower quadrant)
Odynophagia or dysphagia
Flatulence and bloating
Fissures and fistulas
Signs of malabsorption with vitamin B12 and D deficiencies and
iron deficiency anemia
16.
Symptoms:
General manifestations:
• Low-gradefever
• Signs of anemia -
• fatigue
• pallor, dyspnea
• palpitations
• Loss of appetite
• Weight loss
• Failure to thrive or growth delay in children
Diagnosis:
A multimodal approachof clinical features, laboratory investigations ,
endoscopy , Radiology and Pathological findings are required.
Laboratory Studies
• Routine
• Special
Imaging Studies
Tissue diagnosis
• Cytology
• FNAC
• Histology
• Germ line Testing and Molecular Analysis
Diagnostic Laparotomy.
20.
Endoscopy:
Ileocolonoscopy with biopsiesof terminal ileum:-Gold standard.
Sigmoidoscopy or colonoscopy may reveals characteristic aphthous
ulcer with granularity and normal appearing surrounding mucosa.
Presence of discrete ulcers ,cobblestone appearance ,discontinuous
segments of involved bowel favors diagnosis.
Capsule endoscopy also helpful in diagnosis of superficial mucosal
abnormalities.
Management:
Medical Therapy: Directedtowards inducing and maintaining steroid
free remission as well as prevent acute exacerbations and
complications.
It includes:
• Corticosteroids :To treat acute flare of Crohn’s disease.
• Antibiotics: Metronidazole or ciprofloxacin
• Amino salicylates: Colonic symptoms can be treated.
• Immunomodulatory agents:
• Azathioprine: Additive and steroid sparing effects
• Ciclosporin: inhibits cell mediated immunity
23.
Management:
Monoclonal Antibody(Biological) Therapy:
•Induce remission in moderately severe and severe CD
• Infliximab: Murine chimeric anti TNF alpha
• Adalimumab: Entirely human anti TNF alpha Monoclonal Ab.
• Prevent leukocyte migration:
Vedolizumab ,Etrolizumab
• Targets IL 12/23 and dampen immune system
Ustekinumab
24.
Management:
Nutritional therapy:
• Chemicallydefined elemental diet
• Liquid polymeric diet
• Total parenteral nutrition
Smoking Cessation
Balloon dilatation of fibro-stenotic disease may result in substantial
symptomatic improvement and obviate the need for surgery in
selected cases.
25.
Surgical Management:
Goals: Topreserve bowel length ,Minimize post operative
complications and disease recurrence.
Aim:
• Achieve inflammation free margin with minimal surgery
• Intended to remove just grossly inflamed tissue.
• Even if adjacent bowel are clearly diseased ,they should be
ignored.
• Frozen section to be considered only if malignant disease is
suspected.
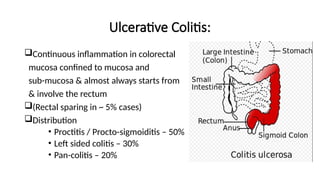
Ulcerative Colitis:
Continuous inflammationin colorectal
mucosa confined to mucosa and
sub-mucosa & almost always starts from
& involve the rectum
(Rectal sparing in ~ 5% cases)
Distribution
• Proctitis / Procto-sigmoiditis – 50%
• Left sided colitis – 30%
• Pan-colitis – 20%
29.
Epidemiology:
The annual incidenceis 10.4-12 cases per 100,000 people, and the
prevalence rate is 35-100 cases per 100,000 people.
Three times more common than Crohn disease
White individuals living in Western industrialized nations
2-4 times higher in Ashkenazi Jews.
The incidence is low in Asia and the Far East.
Symptoms:
Rectal bleeding
Frequent stools
Mucousdischarge from
the rectum
Tenesmus (occasionally)
Lower abdominal pain and severe dehydration from purulent rectal
discharge (in severe cases, especially in the elderly).
32.
Clinical features:
In somecases, UC has a fulminant course marked by the following:
• Severe diarrhea and cramps
• Fever
• Leukocytosis
• Abdominal distention
33.
Signs:
Normal in milddisease
Mild tenderness in the lower left abdominal quadrant
Severe cases-
• Fever
• Tachycardia
• Significant abdominal tenderness
• Weight loss
34.
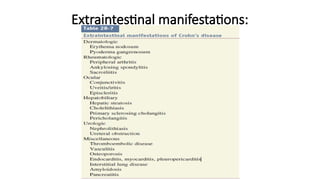
Extra GI Manifestations:
Uveitis
Pyodermagangrenosum
Pleuritis
Erythema nodosum
Ankylosing spondylitis
Spondyloarthropathies
Primary sclerosing cholangitis (PSC)
Recurrent subcutaneous abscesses unrelated to pyoderma gangrenosum
Multiple sclerosis
Immunobullous disease of the skin
35.
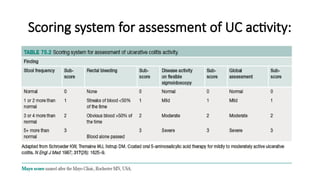
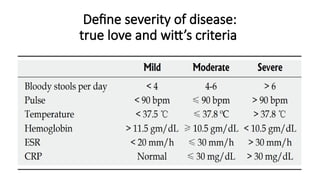
Classification of severity:
Determinedby frequency of bowel action and presence of systemic
signs of illness, Proposed by Trulove and Witt’s:
• Mild: Fewer than four bowel motions per day with or without
bleeding.
• Moderate: More than four bowel motions per day, few signs of
systemic illness, pain abdomen may occur, CRP and ESR raised.
• Severe: More than six bloody stool per day, and a systemic illness
with hypoalbuminemia (< 30 g/L)
• Fulminant : More than ten bowel motions per day with continuous
bleeding ,fever ,tachycardia, anemia,
Hypoalbuminemia ,abdominal distension and tenderness.
36.
Cancer risk incolitis:
The risk of cancer in ulcerative colitis increases with duration of
disease.
At 10 years from diagnosis, it is approximately 1%, increasing to 10–
15% at 20 years and 20% at 30 years.
Patients with pancolitis (defined as the presence of inflammation
proximal to the splenic flexure) of more than 10 years duration should
be entered into endoscopic screening programs in order to detect
clinically silent dysplasia, which is predictive of increased cancer risk.
37.
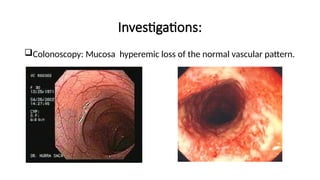
Investigations:
Endoscopy and biopsy:
•Endoscopy and biopsy-Abnormal erythematous mucosa, with or
without ulceration, extending from the rectum to a part or all of the
colon
• Contact bleeding may also be observed, with mucus identified in the
lumen of the bowel
Treatment:
Principles of management:
•Most patients are maintained on optimized medical therapy.
• Acute severe colitis (ASC) requires multidisciplinary management.
• Toxic dilatation or impending complication should be suspected if
the patient develops abdominal tenderness or distension, or
deteriorates clinically
• Patients with colitis are at increased risk of developing cancer;
those with pancolitis of long duration are most at risk
43.
Medical treatment:
Cyclo-oxygenase Inhibitor: 5-Aminosalicylic acid derivatives
topically(per rectal)or systemically.
Corticosteroid either topically or systemically acts as anti
inflammatory.
Immunosuppressive drugs: Azathioprine and ciclosporin
Monoclonal Antibodies: Infliximab , Adalimumab, Ustekinumab
Nutritional support.
44.
Medical treatment ofacute, severe UC :
Hospitalization
Intravenous high-dose corticosteroids
Alternative induction medications: Cyclosporine, Tofacitinib,
tacrolimus, infliximab, adalimumab, golimumab
45.
Indications for urgentsurgery :
Toxic megacolon refractory to medical management
Fulminant attack refractory to medical management
Refractory acute severe colitis
Uncontrolled colonic bleeding by endoscopic or interventional
radiologist team.
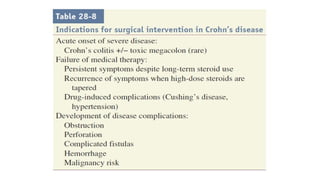
46.
Indications for surgery:
Severeor fulminating disease failing to respond to medical therapy
Chronic disease with anemia, frequent stools, urgency and tenesmus
Steroid-dependent disease where remission cannot be maintained
without substantial doses of steroids with harmful side effects
Intolerance or side effects of medical therapy required to control the
disease, e.g. steroid psychosis, azathioprine induced pancreatitis
●
47.
Indications for surgery:
Growthretardation in children or adolescents
Neoplastic change: patients who have severe dysplasia or carcinoma
Associated sclerosing cholangitis
Extraintestinal manifestations
Rarely, severe hemorrhage or stenosis causing obstruction.
48.
Pre-operative preparation:
Correction of
•Anemia
• Fluid and electrolyte
• Acid-base disorder
• Nutritional deficiencies
Most drugs can be discontinued without sequelae except
corticosteroids
Ostomy site selection
Mechanical Bowel prep – not necessary
Anti-microbial treatment
49.
Surgical Management:
Emergency
• Aim:
•Treatment of fulminant state
• Emergency Surgery:
• Total abdominal colectomy + end ileostomy + rectal stump
closure/fistula
• Able to discontinue all the medication
• Preserve ileal branch of Ileocolic vessel
• Avoid rectum mobilization
50.
Surgical Management:
Elective:
• Subtotalcolectomy and Ileostomy
• Pan-proctocolectomy and permanent end-ileostomy
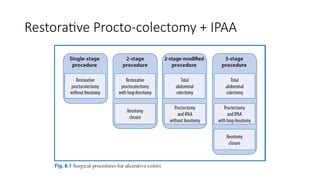
• Restorative proctocolectomy with Ileal pouch-anal
anastomosis(IPAA)
• Sub-total colectomy and ileorectal anastomosis(IRA)
• Segmental Colectomy(Crohn’s Colitis only)
51.
Pan-proctocolectomy and permanentend-
ileostomy
• This operation removes the entire colon and rectum and,
• By doing so, removes any risk of colorectal neoplasia or colitic symptoms
• It results in a permanent ileostomy.
• It has a lower complication rate than an ileal pouch procedure, although
the perineal wound can be problematic (10% fail to heal) and stoma
problems are common.
• It is indicated for patients who are not candidates for restorative surgery
owing to impaired anal sphincter function, comorbidities or patient
preference
52.
Total procto-colectomy +Brooke ileostomy
Indications
• Old age / anal incontinence
• Distal rectal Ca
• Patient preference
Disadvantage
• Loss of fecal continence
• SAIO
53.
Total procto-colectomy +Continent ileostomy
Indication
• As Brooke ileostomy
Operative principles
• Exclude CD
• Aperistaltic reservoir
• Terminal 45-60 cm of the ileum – S pouch
• Early post-op - wide plastic tube drain in the pouch
• Drainage -- by intubating the pouch 3 times/D
Abdominal Colectomy +IRA
Indication
• Indeterminate colitis (IC)
• Upper rectal disease- rectal compliance remains adequate
Advantage
• Avoid perineal complication of proctocolectomy
• Minimal sexual dysfunction/ fertility
• Control of feces and flatus
59.
Abdominal Colectomy +IRA:
Disadvantage
• Rectal mucosa remaining
• Increased frequency of defecation – 2-5 times/d, semi-liquid
• Conversion to IPAA
• Poor rectal compliance
• Persistent proctitis
• Upper rectal Ca
60.
Abdominal Colectomy +IRA:
Complication
• Nocturnal defecation
• Ca risk ( In remaining rectum)
• Overall risk – 6%
• Most Ca. appear 15-20 yrs. after operation
• Recurrent or persistent inflammation
• Incidence – 20%-45%
• Severe diarrhea, tenesmus, bleeding, urgency
• Topical or systemic therapy – if no response – rectal excision
61.
Controversial issue inSurgical Management:
Indeterminate colitis- In 10% colitis patients
• Overlapping features of UC & CD
• If CD cant be excluded – subtotal colectomy + ileostomy
• IPAA for IC
• Definitive pathologic diagnosis of UC
• IC without development of signs or symptoms of CD
• Long term functional outcome nearly identical to chronic UC
• Pouch loss
• Higher perineal complications
• IPAA for UC/IC
• 7% have revised diagnosis of CD
• High rate of perianal fistula / stricture
62.
Take home message:
•Crohn's disease is a chronic, recurrent condition that causes patchy
transmural inflammation that can involve any part of the
gastrointestinal tract.
• Diagnosis is established via endoscopy with biopsy that shows
transmural inflammation, characteristic “cobblestone” mucosa, and
noncaseating granulomas.
• Management is with corticosteroids, azathioprine, antibiotics, and
anti-TNF agents (infliximab and adalimumab).
• Complications include malabsorption, malnutrition, intestinal
obstruction or fistula, and an increased risk of colon cancer.
63.
Take home message:
•UC is generally limited to the colon, apart from minimal distal "back-
wash" ileitis;
• Ulcerative colitis usually involves only the mucosal layer of the bowel,
and, in some cases, superficial submucosa, unless there is fulminant
colitis
• May also manifest caecal or appendiceal patches of involvement that
can simulate the "skip" lesions of CD
64.
References:
• Bailey andlove’s short practice of surgery-28th
edition
• Sabiston textbook of surgery-21st
edition
• Schwartz’s principles of surgery 11th
edition
• British Society of Gastroenterology consensus guidelines on the
management of inflammatory bowel disease in adults; 2019
Editor's Notes
#4
Both UC and CD occur in individuals who may have a genetic predisposition and who are exposed to environmental factors that trigger abnormal immune responses that lead to intestinal infammation
#6
1.frequently diagnosed between the ages of 25 and 40 years. There is a second peak of incidence around the age of 70 years
#7 In addition,
dysbiosis with a decrease in intraluminal Bacteroides and
Firmicutes and an increase in Gammaproteobacteria and Actinobacteria
are associated with higher risk.
#8 1. Attention has focused on the role
of cytokines, such as interleukin (IL)-1, IL-2, IL-8, and TNF-α,
as contributing factors in the intestinal inflammatory response.
2.Genetic factors:single strongest risk
factor for development of disease is having a first-degree relative
with Crohn disease.
3.NOD Genes associated with a decreased expression of antimicrobial peptides
by Paneth cells..
4. A complex cellular and molecular crosstalk occurs between
the genes NOD2/CARD15 and the autophagy gene ATG16L1,
which is associated with a synergistic increase in earlier onset
and disease severity
5.Smoking: single nucleotide polymorphism occurs.
#12
1.Oedema between ulcers gives rise to a characteristic cobblestone appearance of the mucosa
2.
The trans-mural infammation (a pathognomonic feature of CD) may lead to segments of bowel becoming adherent to each other and to surrounding structures, forming infammatory masses with mesenteric abscesses and fstulation into adjacent
#19 1. Complete blood count will show anemia, leukocytosis, and thrombocytosis.
Complete metabolic panel to check if chronic diarrhea has caused electrolyte imbalance
Iron deficiency and vitamin B deficiency
↑ ESR and CRP
Stool studiesMay be used to exclude other causes of inflammatory diarrhea(e.g., infection)
Clostridioides difficile toxin studies in cases of recent antibiotic use
May show traces of blood in the stool
2. X-Ray
USG
CT
Angiography
MRI
Endoscopy
Nuclear scan
#20 1. The most commonly
used criterion for an abnormal finding is the presence of
three or more ulcers in the absence of NSAID use. The use of
this modality is limited because of concern for capsule retention,
defined as the presence of the capsule in the gastrointestinal tract
for more than 2 weeks, which is of greater concern to patients
with Crohn disease due to a significantly higher risk of retention
(13%)
#22 1.
Metronidazole and ciprofoxacin may be used, particularly for periods of a few weeks at a time, especially in perianal disease. Long-term use of metronidazole should be avoided as there is a risk of peripheral neuropathy. Ciprofoxacin also has signifcant side efects when used in the long term, including tendinitis and tendon rupture.
2.
Azathioprine is used for its additive and steroid-sparing efects and currently represents standard maintenance therapy. It is a purine analogue, which is metabolised to 6-MP, and works by inhibiting cell-mediated immune responses
#25 1.Chronic Crohn's disease will require surgery at some point of Illness. Approx. 70% patient will require surgical intervention within 15 years of diagnosis.
#28 1.Characterized by mucosal inflammation of large bowel, always involving the rectum and extending to involve varying degrees of more proximal colon.
Chronic condition that tends to be relapsing and remitting.
Early relapse and persistent disease within 2 years of diagnosis are predictors of severe disease course.
#29 1.As new regions assume Western cultural practices, an increased prevalence of ulcerative colitis is usually found approximately 1 decade before the observed increase in Crohn disease.
#35 Fulminant:
the need for blood transfusion and, in the most severe cases, progressive colonic dilation (toxic megacolon). This is a very signifcant fnding, suggestive of disintegrative colitis, and an indication for emergency surgery if colonic perforation is to be avoided.


![Investigations:
• Serologic markers (eg, antineutrophil cytoplasmic antibodies [ANCA],
anti– Saccharomyces cerevisiae antibodies [ASCA])
• Complete blood cell (CBC) count
• Comprehensive metabolic panel
• Inflammation markers (eg, erythrocyte sedimentation rate [ESR], C-
reactive protein [CRP])
• Stool assays: To exclude infective colitides, notabely Camphylobacter](https://image.slidesharecdn.com/inflammatoryboweldiseasesujanpptx-250525023511-e0429a45/85/Inflammatory-Bowel-Disease-sujan-pptx-pptx-39-320.jpg)