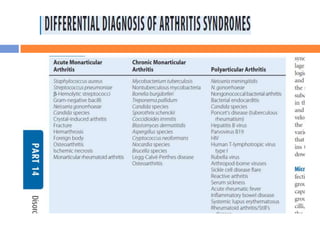
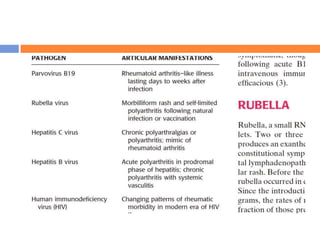
This document discusses various types of infectious and viral arthritis. Septic arthritis is a potentially life-threatening joint infection most often caused by bacteria entering the joint from another infected site. Diagnosis involves joint fluid analysis showing very high white blood cell counts. Treatment requires antibiotics and sometimes surgery. Risk factors include age, diabetes, and prosthetic joints. Parvovirus B19 and rubella can also cause self-limiting viral arthritis mimicking rheumatoid arthritis.

![Diagnosis
Arthrocentesis and synovial fluid analysis
are the cornerstones for the diagnosis of
septic arthritis.
If the synovial fluid white blood cell (WBC)
count is extremely high [e.g., >100,000/mm3
white blood cells (WBC)], treatment for
presumed septic arthritis should be
initiated pending culture result of the fluid.](https://image.slidesharecdn.com/infectionsandarthritis-130401020156-phpapp01/85/Infections-and-arthritis-9-320.jpg)





































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

