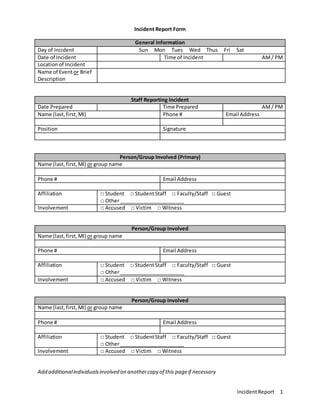
The document details an incident report form used for documenting various types of incidents, including accidents, assaults, and policy violations. It requires general information about the incident, individuals involved, and the nature of the response. The form also includes sections for follow-up and additional notes if necessary.