Downloaded 1,193 times
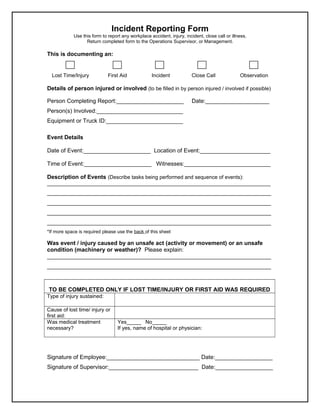

An incident reporting form is used to document any workplace accidents, injuries, incidents, close calls, or illnesses. The completed form should be returned to the Operations Supervisor or Management. The form collects details of the injured person if applicable, the person completing the report, event details including location and witnesses, and a description of the sequence of events. For lost time injuries or those requiring first aid, additional details are collected including the type of injury sustained, cause of the injury or incident, and whether medical treatment was necessary.







![[Letter of Appointment] Chemsain Konsultant Sdn. Bhd. - Member of the Emergen...](https://cdn.slidesharecdn.com/ss_thumbnails/713a183a-605d-4578-8415-ad84d4a5aec3-160802040716-thumbnail.jpg?width=640&height=640&fit=bounds)

































































