Downloaded 59 times












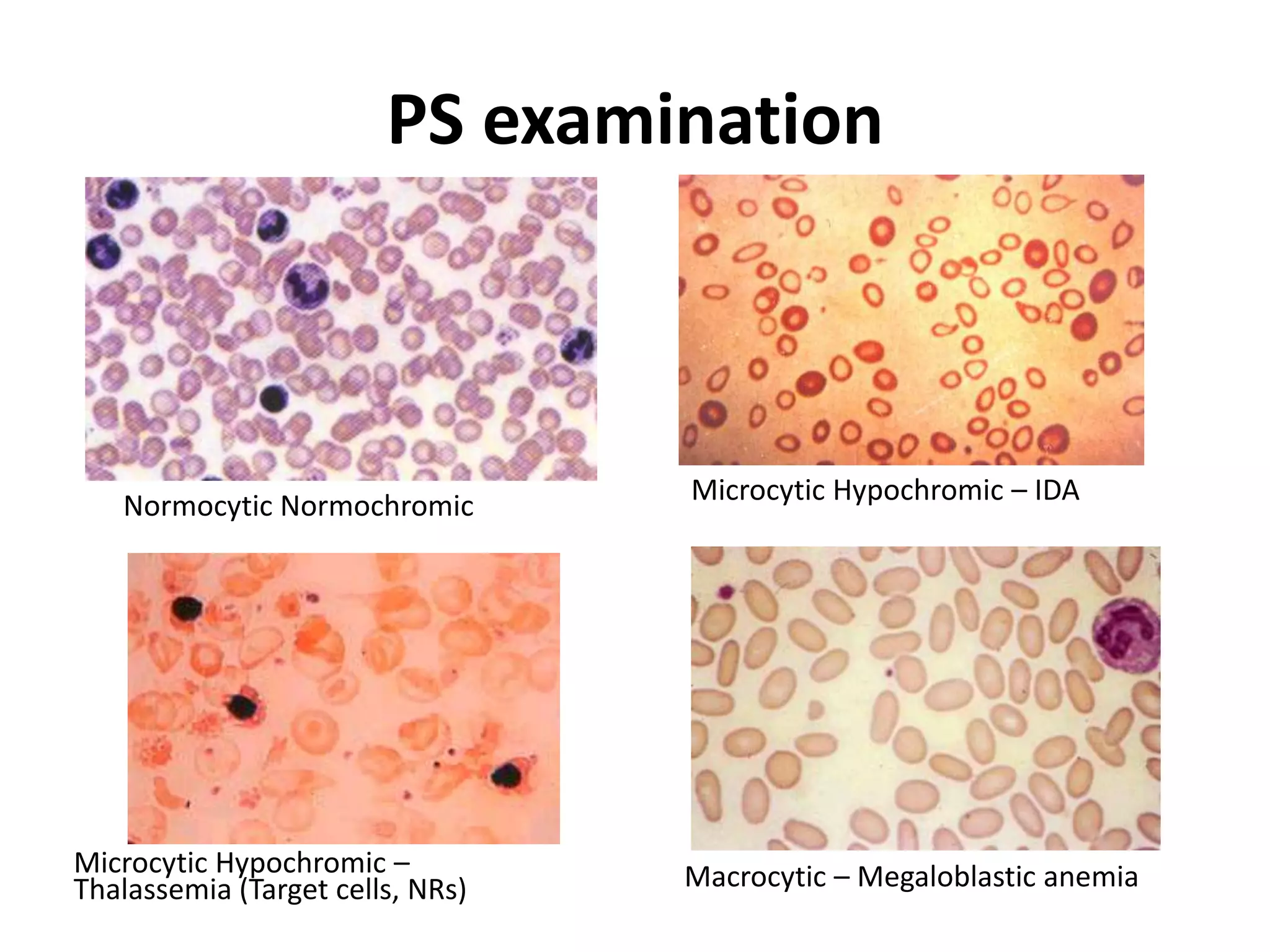







Hypochromic anemia is a type of anemia where red blood cells appear paler than normal. There are two main classifications - iron deficiency anemia and non-iron deficiency anemia which includes conditions like sideroblastic anemia, thalassemia, and anemia of chronic diseases. Iron deficiency anemia is caused by low iron intake, decreased absorption, blood loss, drugs, or transport defects. Clinical evaluation involves taking a thorough history and conducting a physical exam looking for pallor, nail changes, enlarged spleen or liver, and cardiovascular abnormalities. Investigations help determine the severity through tests like hemoglobin, ferritin, and peripheral smear examination. Treatment depends on the underlying cause but commonly involves oral or
















































































