The document discusses thyroid disorders, detailing the evaluation, causes, symptoms, complications, and treatments of both hypothyroidism and hyperthyroidism. It covers specific conditions like Graves' disease, explains diagnostic methods, and describes the management of serious complications such as myxedema coma and thyrotoxic crisis. Additionally, it highlights the historical advancements in surgical techniques related to thyroid disorders.
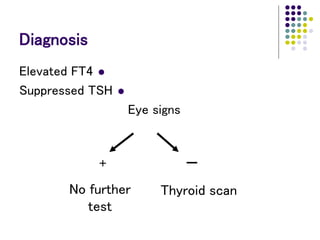
![Diagnosis
TSH-R Ab [stim]
Free T3
Atypical presentations:
- Thyrotoxic periodic paralysis
- Thyrocardiac disease
- Apathetic hyperthyroidism
- Familial dysalbuminemic hyperthyroxinemia](https://image.slidesharecdn.com/16-hypoandhyperthyroidism-230119130607-78cda9d7/85/Hypo-and-Hyperthyroidism-ppt-38-320.jpg)
![Surgical advances
1866
“If a surgeon should be so foolhardy as to undertake it
[thyroidectomy] … every step of the way will be
environed with difficulty, every stroke of his knife will
be followed by a torrent of blood, and lucky will it be
for him if his victim lives long enough to enable him to
finish his horrid butchery.”
– Samuel David Gross](https://image.slidesharecdn.com/16-hypoandhyperthyroidism-230119130607-78cda9d7/85/Hypo-and-Hyperthyroidism-ppt-52-320.jpg)