Downloaded 61 times
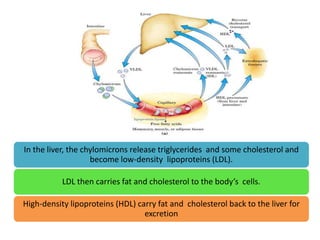
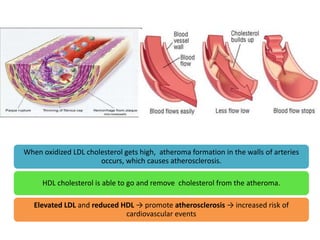
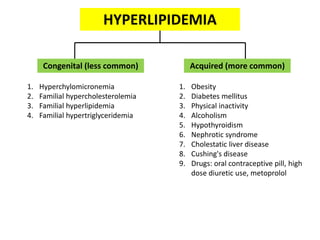
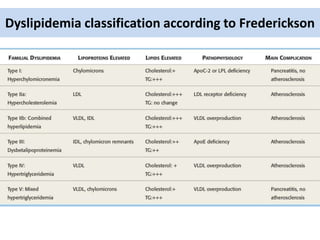




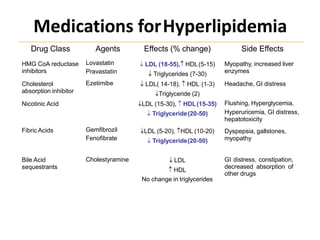
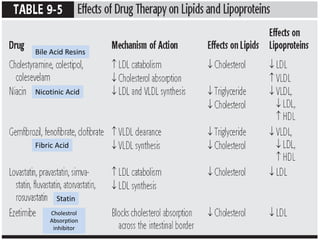

Hyperlipidemia is defined as elevated levels of total cholesterol, LDL cholesterol, or triglycerides. It is a major risk factor for atherosclerosis and cardiovascular disease. LDL carries cholesterol to tissues while HDL removes cholesterol from tissues and returns it to the liver. Elevated LDL and reduced HDL promote atherosclerosis. Hyperlipidemia can be caused by genetic factors, obesity, diabetes, hypothyroidism, and certain drugs. It is investigated through a fasting lipid profile and classified using the Frederickson system. Treatment involves lifestyle modifications and medications like statins, fibrates, nicotinic acid, and bile acid sequestrants.











































































