Downloaded 63 times
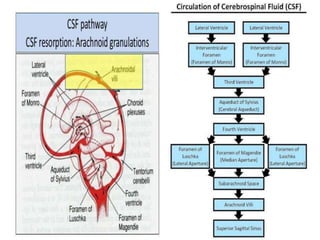
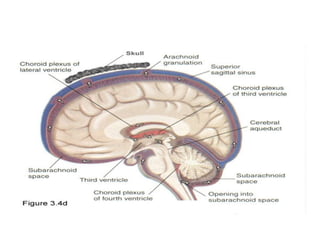
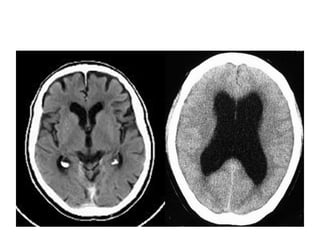

Hydrocephalus is defined as an imbalance between cerebrospinal fluid (CSF) production and absorption, leading to various causes including congenital malformations and external factors like infections or trauma. It is categorized into non-communicating and communicating types, each with distinct pathophysiological mechanisms and clinical manifestations in infants, children, and adults. Management options include medical therapies to reduce CSF production and surgical interventions such as shunt placement and endoscopic procedures to restore normal CSF flow.




![Fetal birth-injuries[1]](https://cdn.slidesharecdn.com/ss_thumbnails/fetal-birth-injuries1-121204143707-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




































































