Downloaded 250 times

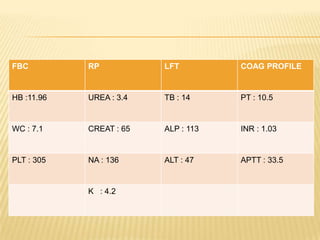
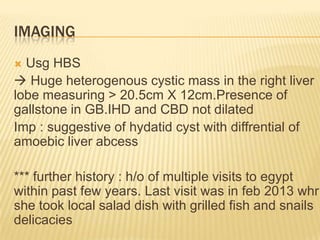
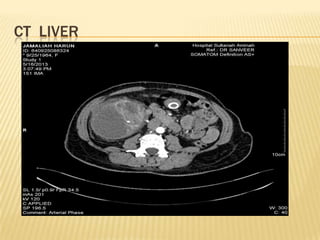

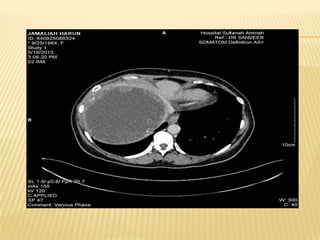
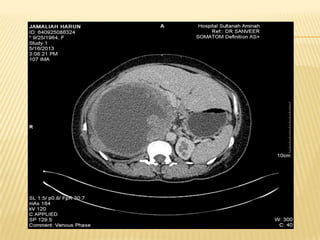
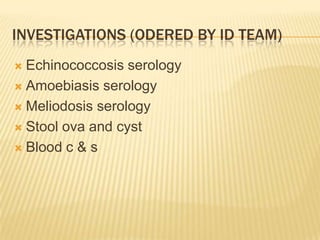

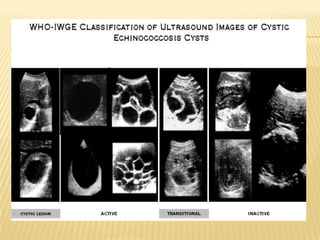

This case report describes a 49-year-old woman who presented with abdominal pain and weight loss. Imaging revealed a large cystic mass in her liver consistent with a hydatid cyst. She was treated with albendazole and referred for surgery. Hydatid disease is caused by the tapeworm Echinococcus and commonly involves the liver or lungs. Diagnosis involves history, imaging, and serology. Treatment options include medical therapy with albendazole or surgery to remove the cyst. Percutaneous aspiration, injection and re-aspiration (PAIR) is a minimally invasive alternative to surgery but has a higher risk of allergic reactions.











































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









