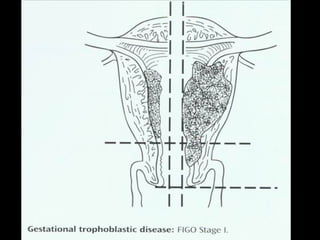
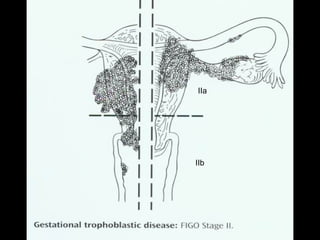
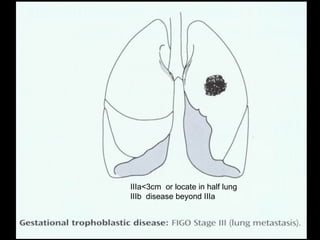
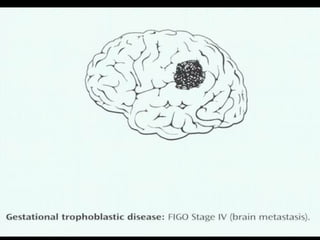
This document discusses gestational trophoblastic disease (GTD), including types like hydatidiform mole. It provides details on:
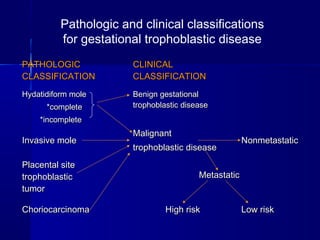
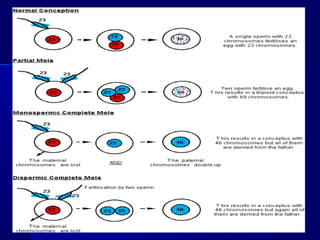
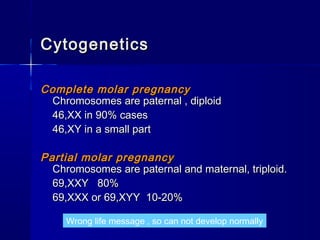
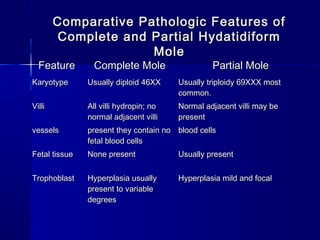
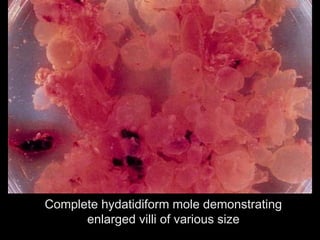
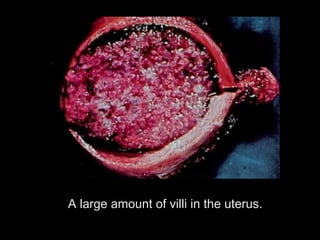
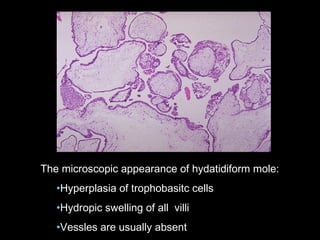
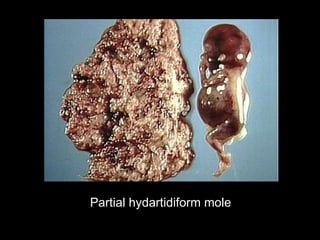
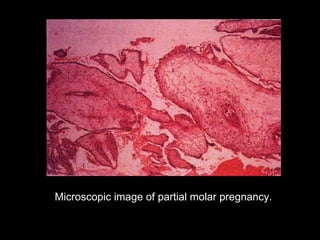
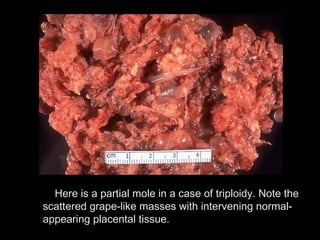
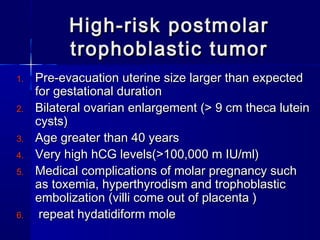
- Hydatidiform mole (molar pregnancy) which is characterized by vesicular swelling of placental villi and absence of an intact fetus. It can be complete or partial.
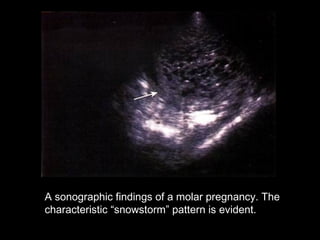
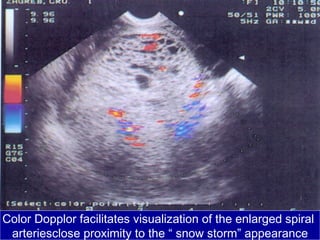
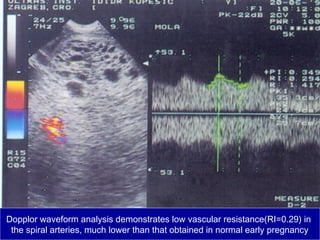
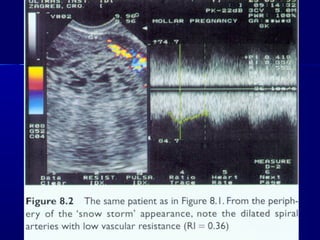
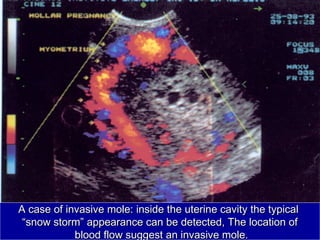
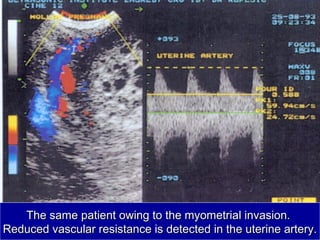
- Diagnosis involves quantitative beta-HCG testing and ultrasound showing a "snowstorm" pattern. Symptoms include vaginal bleeding.
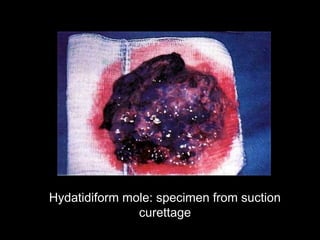
- Treatment is suction dilation and curettage to remove benign hydatidiform moles. Precautions like oxytocic agents after evacuation are recommended.























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







