Downloaded 344 times





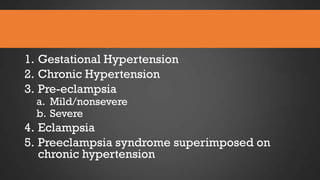
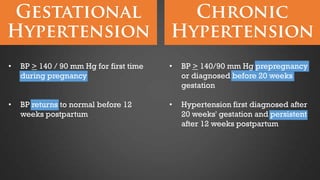
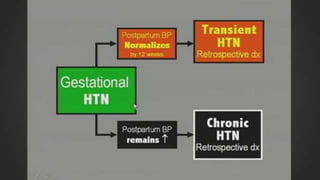

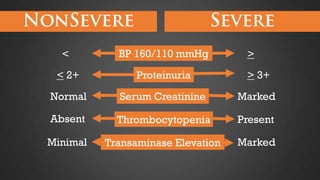
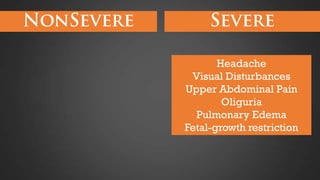








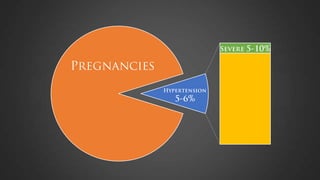
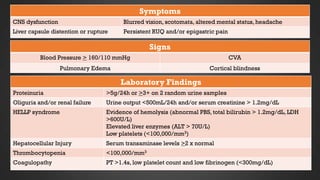
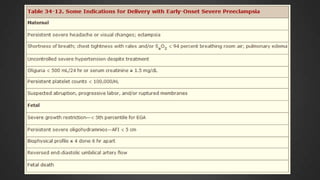


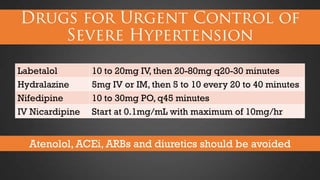
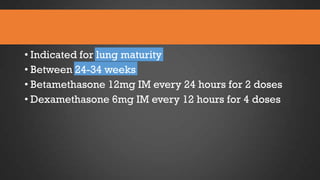

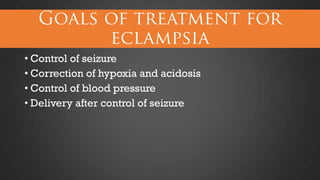


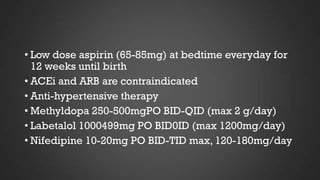





This document discusses hypertensive disorders of pregnancy, which complicate 5-10% of pregnancies. It defines various types of hypertensive disorders including gestational hypertension, chronic hypertension, preeclampsia, eclampsia, and preeclampsia superimposed on chronic hypertension. It outlines diagnostic criteria and management guidelines for each disorder. Key points covered include definitions, risk factors, complications, treatment and delivery timing based on gestational age. The goal of management is to ensure the safety of the mother and fetus.

















![H:\Gestational Hypertension Capp Moms Mess 2[1]](https://cdn.slidesharecdn.com/ss_thumbnails/hgestationalhypertensioncappmomsmess-21-100304134429-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)





































































