Downloaded 348 times



















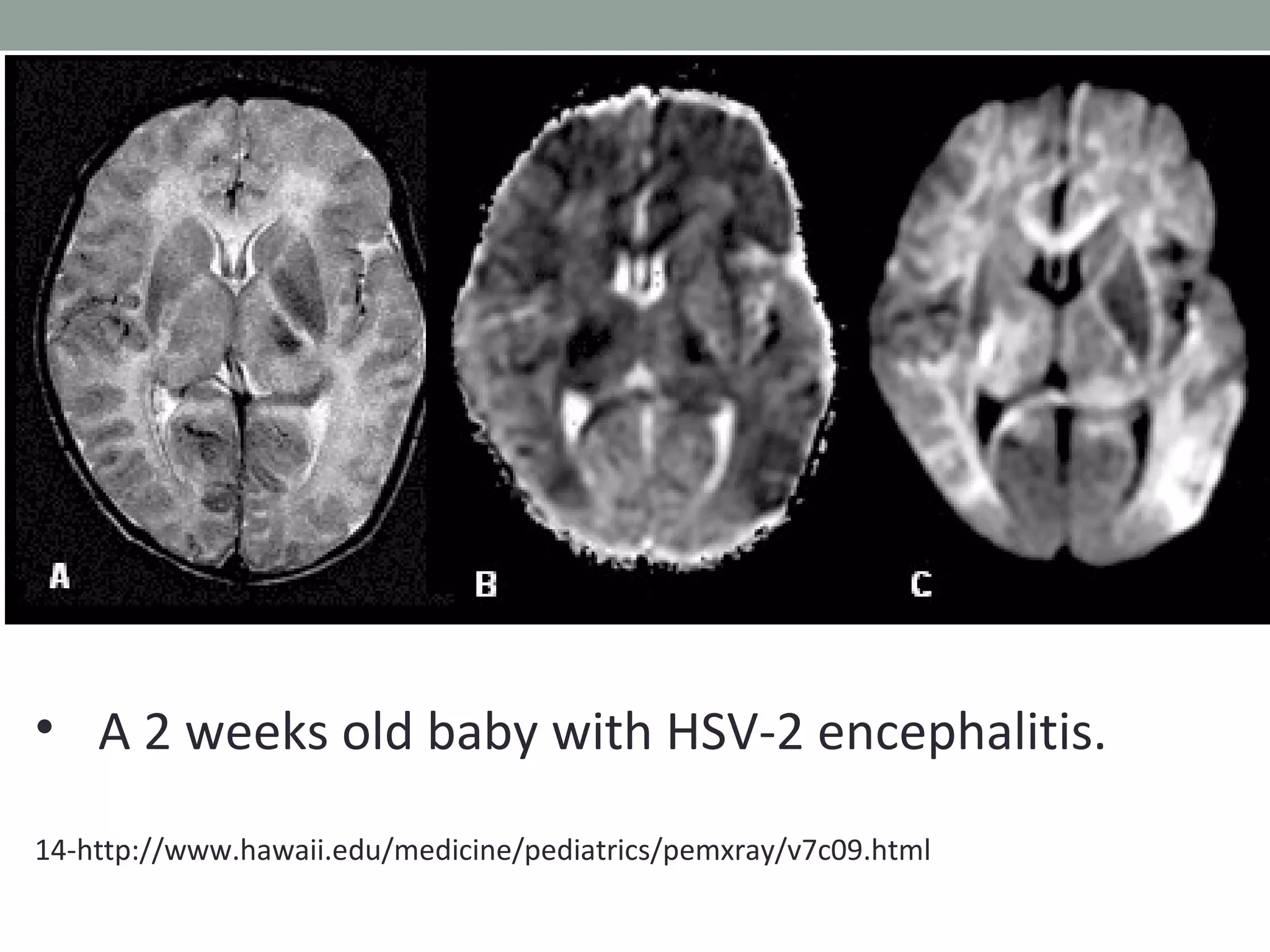


































This document provides an overview of herpes simplex encephalitis (HSE). It discusses the etiology, epidemiology, pathophysiology, clinical manifestations, diagnosis and treatment of HSE. Key points include: HSE is most commonly caused by HSV-1 and is a leading cause of viral encephalitis in children; presentation varies from non-specific symptoms to seizures, altered mental status and focal neurological deficits; diagnosis involves CSF analysis, neuroimaging and PCR testing; and treatment involves high-dose intravenous acyclovir administered for at least 21 days. Recurrence of HSE is possible due to viral reactivation or immune-mediated processes.




















































































