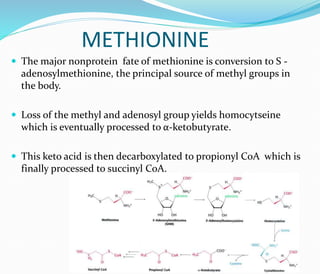
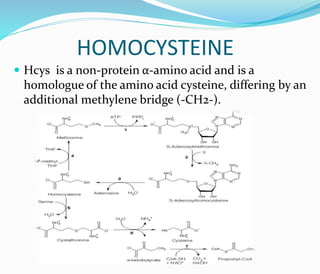
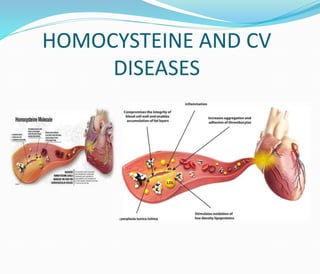
This document discusses methionine metabolism and homocysteine (Hcys). It notes that methionine is converted to S-adenosylmethionine, which provides methyl groups. This reaction yields Hcys, which is processed through remethylation or transsulfuration pathways requiring various B vitamins and minerals. Elevated Hcys is a risk factor for cardiovascular disease and can be caused by genetic defects, nutrient deficiencies, or alcohol use. Treatment focuses on supplementing deficient B vitamins and other cofactors to support Hcys processing and lower risk.














































![Amino-Acid Metabolism [Methionine].pptx..](https://cdn.slidesharecdn.com/ss_thumbnails/amino-acidmetabolismmethionine-241015153732-4ddd3f27-thumbnail.jpg?width=640&height=640&fit=bounds)














![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












