This document discusses several common gastrointestinal defects in children, including cleft lip and palate, exomphalos, and esophageal atresia.
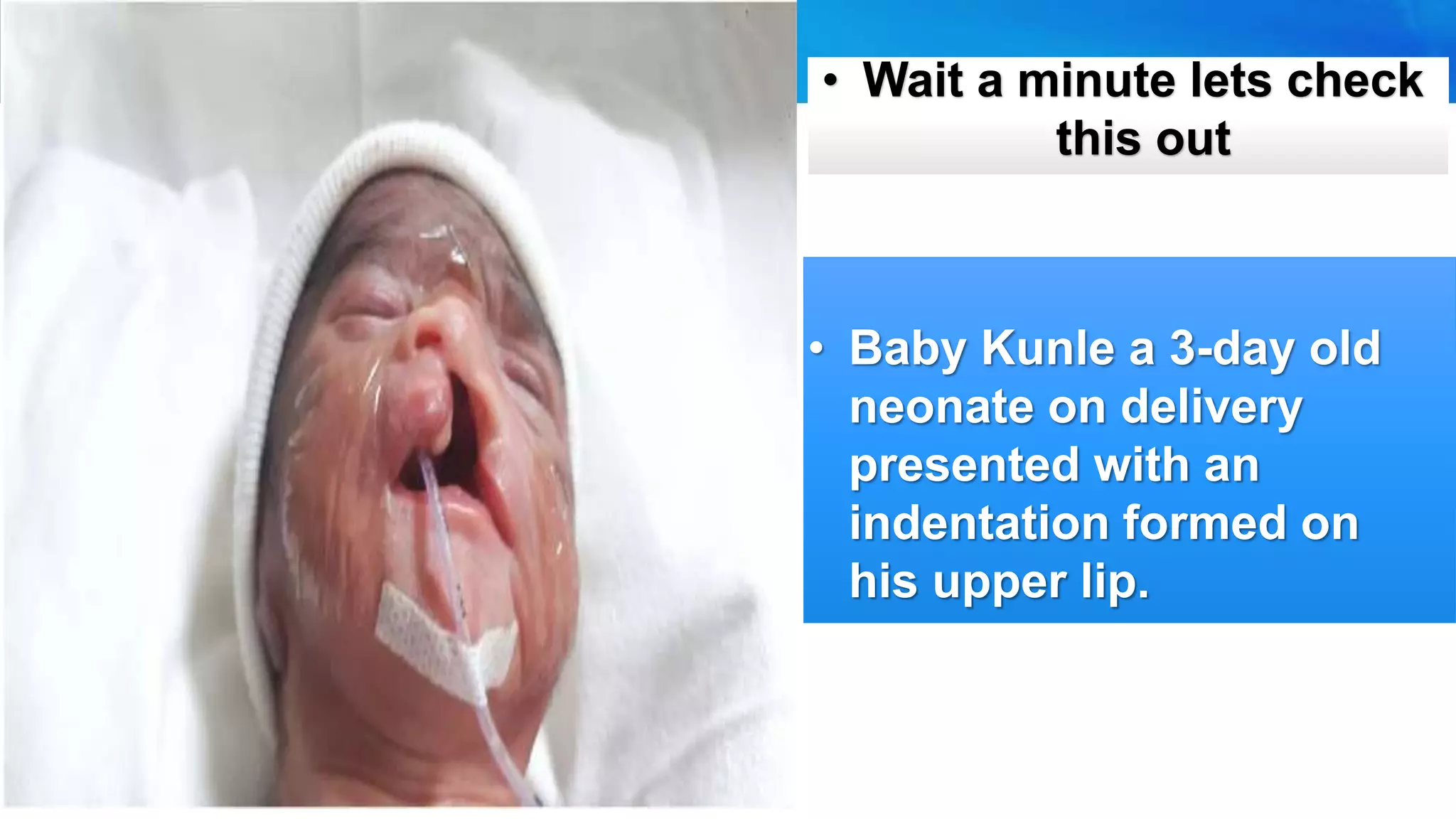
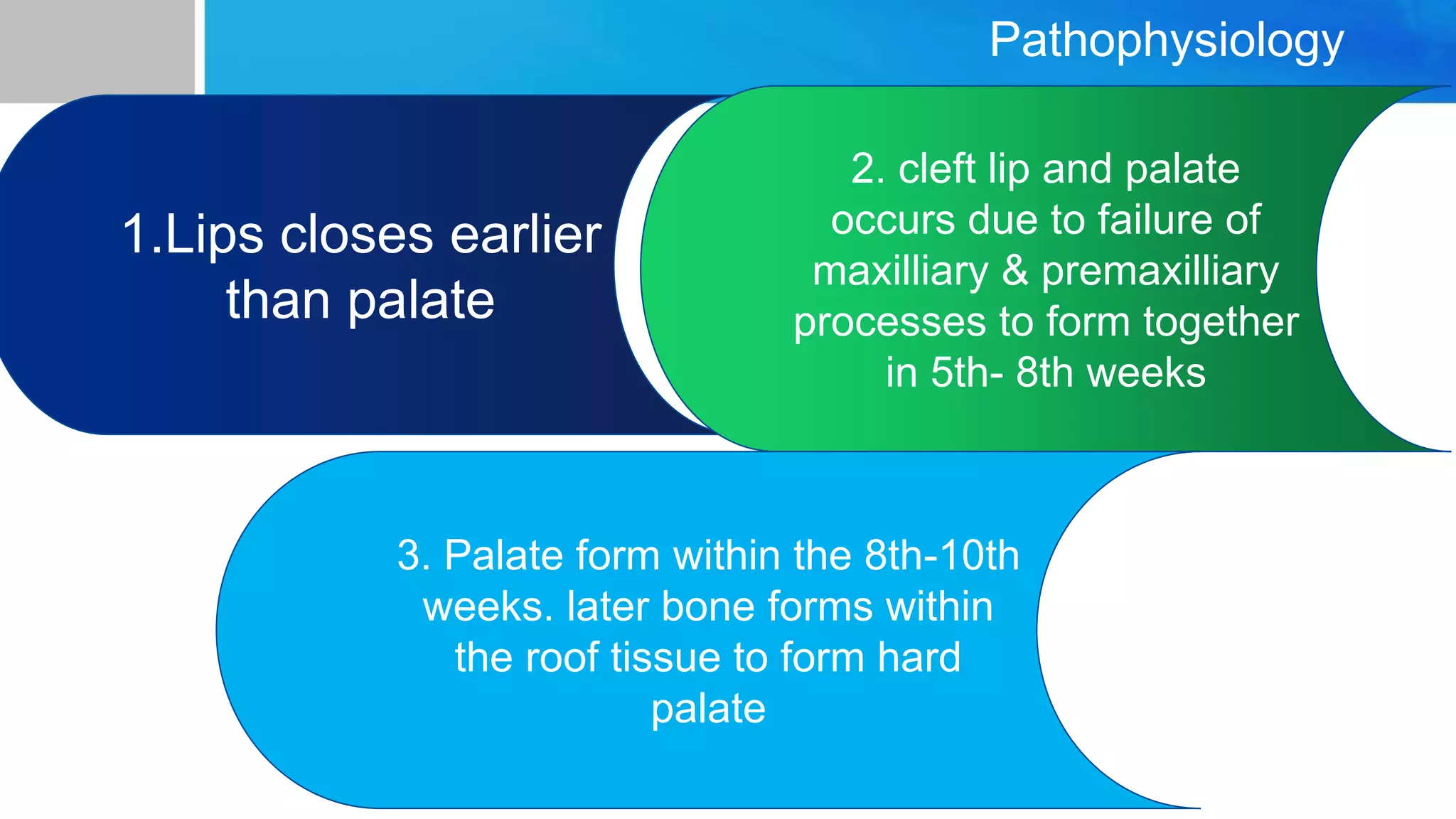
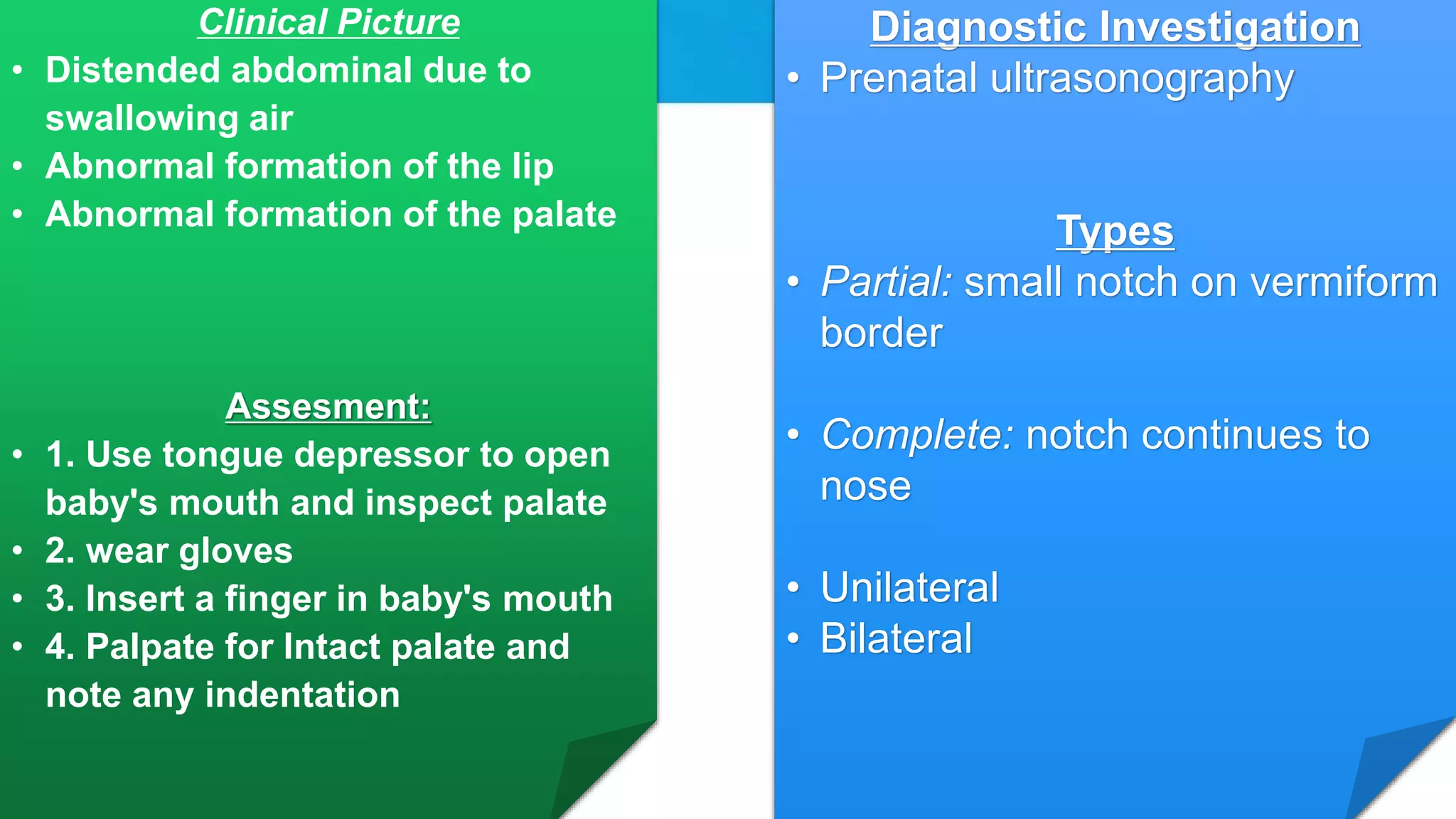
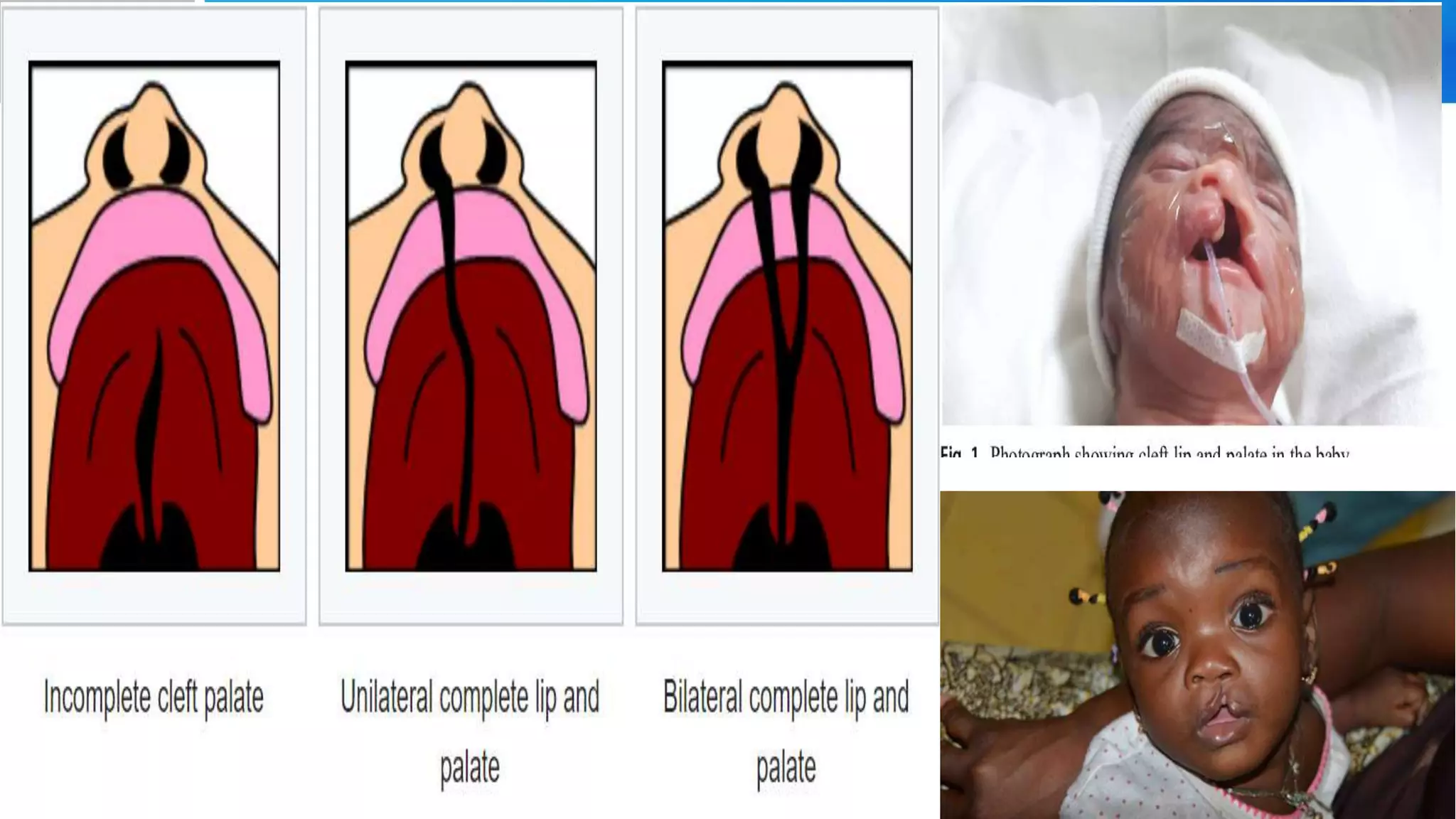
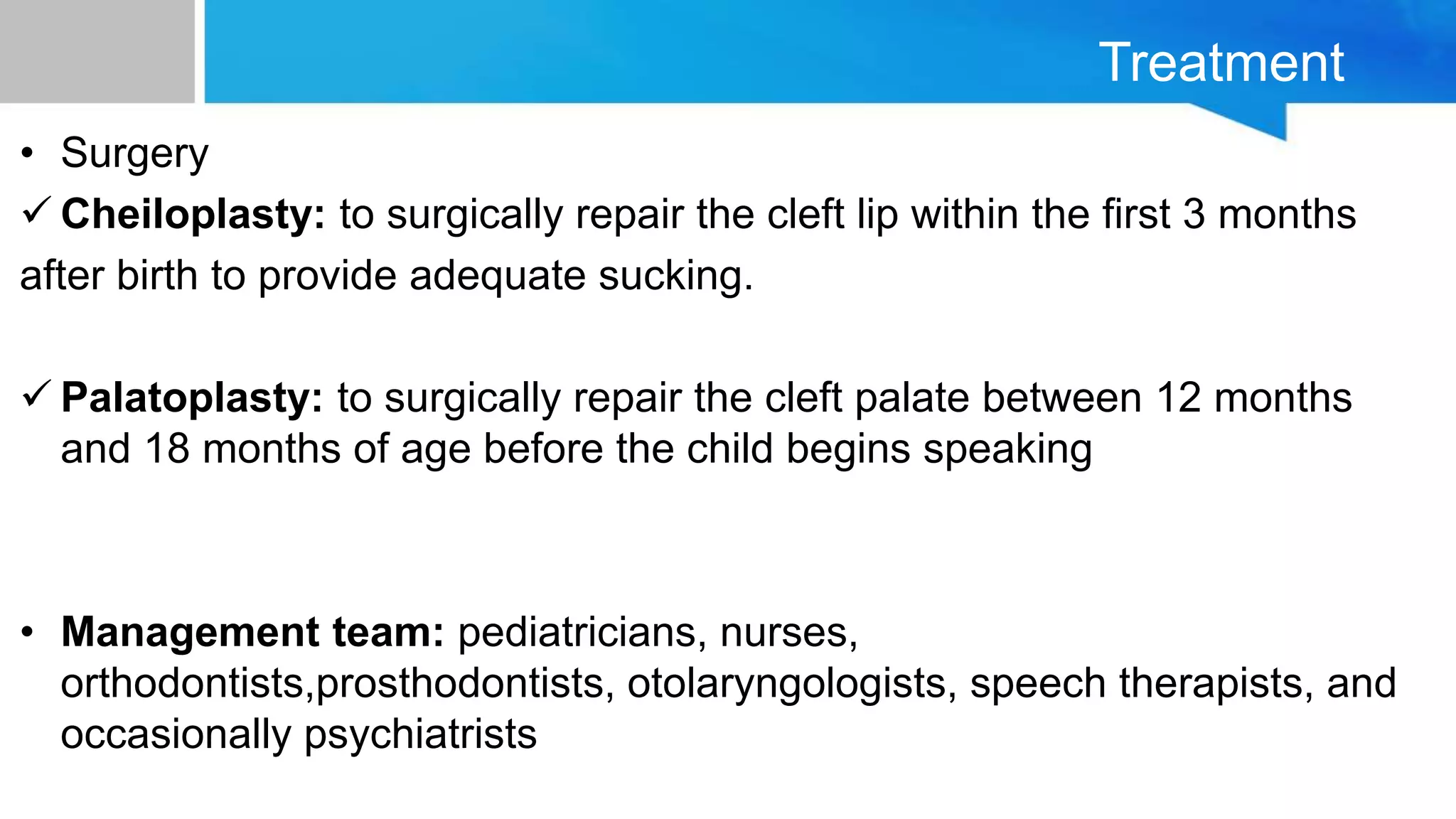
It describes Baby Kunle, a 3-day old with a cleft lip, and provides details on the causes, incidence, pathophysiology, clinical presentation, diagnosis, and treatment of cleft lip and palate. Surgical repair is usually done in the first few months of life. Nursing care involves careful feeding and psychosocial support.
Exomphalos, or omphalocele, is defined as herniation of abdominal contents through the umbilical ring. It has a low incidence. Surgical repair aims to replace organs into the abdomen










![Gastroschisis
• In gastroschicis the exposed bowel is covered loosely
with saline soaked pads and the abdomen is losely
wraped with plastic (rubber) bag or drape or silo bag
• Tight wrapping causes pressure on the expanding organs
and could result in necrosis]](https://image.slidesharecdn.com/nurs342medicalgroup9-200223180626/75/Omphalocele-Exomphalos-cleft-palate-Oesophageal-atresia-and-Nursing-care-37-2048.jpg)