Downloaded 146 times



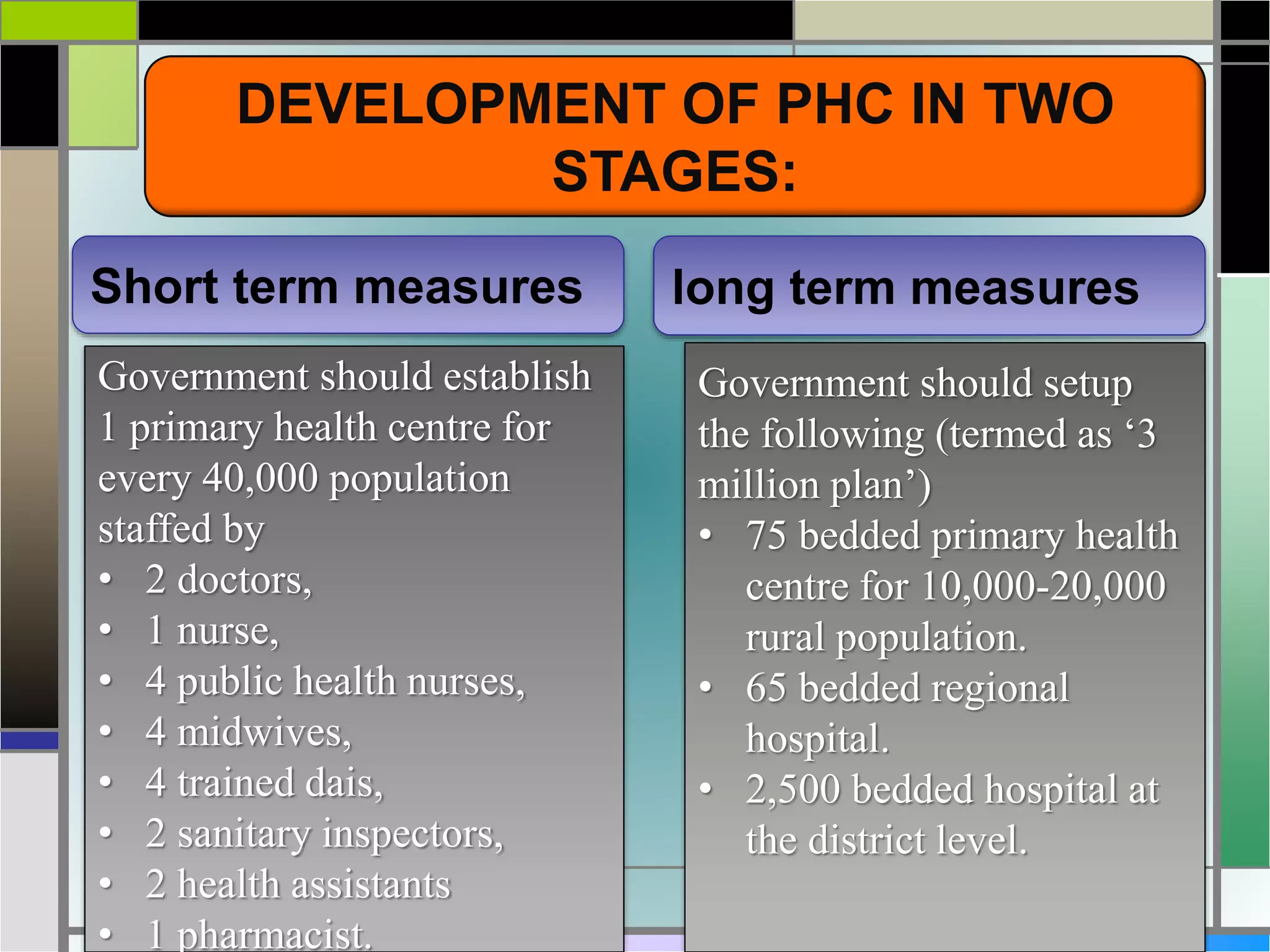














The document outlines various health and family welfare planning committees constituted by the Government of India from 1946 onwards. It discusses the key recommendations and objectives of committees like the Bhore Committee (1946), Mudaliar Committee (1962), Chadha Committee (1963), Mukherji Committee (1965, 1966), Jungalwalla Committee (1967), Kartar Singh Committee (1973), Shrivastav Committee (1975), and others up to the Krishnan Committee (1992). The committees were aimed at reviewing India's health situation and recommending measures to strengthen primary healthcare, integrate services, and achieve the goal of 'Health for All' by 2000.






















































































