Download as PDF, PPTX

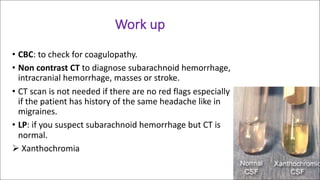


This document provides guidance on evaluating patients presenting to the emergency department with headaches. It emphasizes taking a thorough history including details on headache onset, progression, severity and associated symptoms. The examination should include a neurological exam checking cranial nerves, eye movements, and sensation. Common differential diagnoses are discussed like subarachnoid hemorrhage, meningitis, migraine and tension headaches. Recommended workup depends on risk factors and may include CT, MRI or lumbar puncture. Special considerations for pediatric patients are also reviewed.















































































