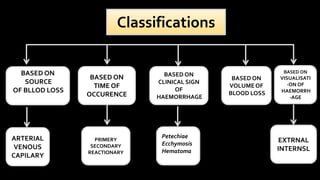
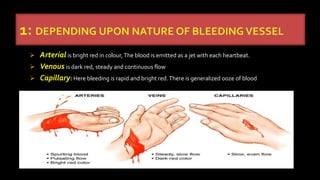
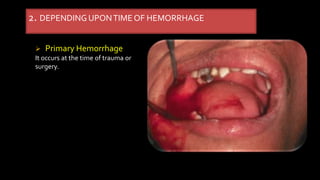
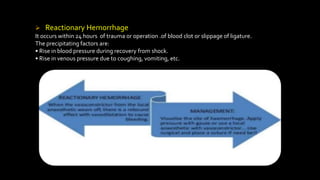
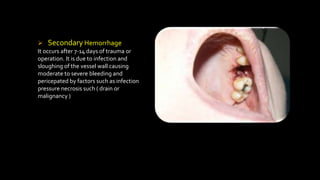
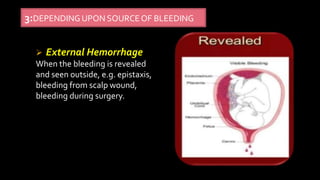
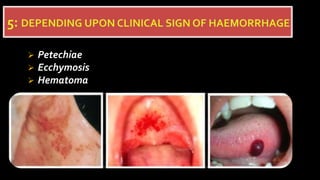
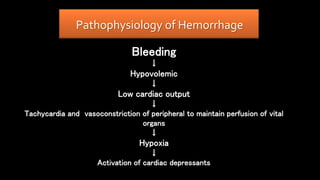
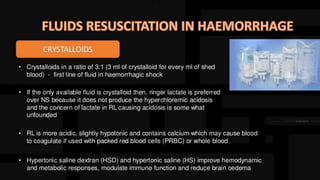
The document provides a comprehensive overview of hemorrhage, including its definitions, classifications by source and time of occurrence, and various types based on volume and speed of blood loss. It also outlines the causes, pathophysiology, clinical features, and hematological investigations relevant to hemorrhage. Key clinical features of acute blood loss and potential laboratory tests for diagnosis are highlighted.