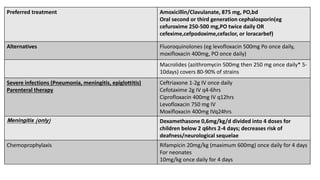
Haemophilus influenzae is a Gram-negative coccobacillus that commonly infects the human respiratory tract and can cause serious invasive disease. The most virulent strain is type b, which most commonly causes meningitis in young children. Symptoms of H. influenzae infection vary depending on the site of infection but may include fever, respiratory distress, and neurological dysfunction. Treatment involves antibiotics like ceftriaxone. Routine vaccination against H. influenzae has dramatically reduced the incidence of invasive disease in countries where it is part of the standard childhood vaccine schedule.














































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








