



![Psychosocial (Erick Erickson)
[Sense of trustVs Mistrust]
Trust – Firm believing the reliability, truth or
ability of someone or something
Mistrust – Lack of trust or confidence; distrust.
Complete dependence on care giver](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-41-2048.jpg)
![Psycho sexual (Freud)
[Oral stage] –This is the first social and sexual
stage of an infant’s development, during
which the infant focuses on satisfying hunger.
This is satisfied by chewing, sucking and
biting.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-42-2048.jpg)
![Spiritual development: (Fowler)
[Undifferentiated] – Feeling of trust, warmth
and security from the foundation of the later
development of faith.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-43-2048.jpg)
![Intellectual development: (Jean Piaget)
[Sensory motor] (0-2 years)
Stimuli are recognized, absorbed and
incorporated into existing action.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-44-2048.jpg)
![Moral development: (Kohlberg)
[Pre-conventional morality stage] (0-2 years)
Unable to understand good or bad
The good is what I like and want](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-45-2048.jpg)
![Play: (New Hall)
[Solitary play]Alone; without companions;
done without assistance or accompaniment
Infants can play alone for longer periods.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-47-2048.jpg)
![Psycho social (Erick Erickson)
[AutonomyVs Shame]
Autonomy – The right of a person, an
organization, region etc.
Shame – The unpleasant feeling of guilt and
embarrassment that you get when you have
done stupid or morally wrong.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-52-2048.jpg)
![Psycho sexual (Freud)
[Anal stage] – Obtain pleasure from the feeling
of a distended bladder, from masses of feaces
in the rectum and from release of content
from those organs.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-53-2048.jpg)
![Spiritual development (Fowler)
[Intuitive projective] – Imitates religious
behavior such as bowing the head in prayer,
but does not understand the meaning.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-54-2048.jpg)
![Moral development (Kohl berg)
[Pre conventional morality stage]
Birth to 2 yrs –The good is what the child like
and wants
2 to 3 yrs – Child is punished for doing
something, its wrong; if not punished it must
be right.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-56-2048.jpg)
![Play (New Hall)
[Parallel play] – A form of play in which a very
young child plays independently in the
presence of another child or children.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-58-2048.jpg)
![Psychosocial (Erick Erickson)
[Sense of initiativeVs Guilt]
Initiative – An introductory act or step; leading
action.
Guilt – A feeling of responsibility or remorse for
some offense, crime, wrong
Independent and trust worthy, they are ready to
find out what they can do.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-64-2048.jpg)
![Psycho sexual (Freud)
[Phallic stage]
Oedipus complex – Boys desire their mothers
while experiencing an increased hostility
towards their fathers.
Electra complex – Girls want their fathers and
find their mothers in their way.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-65-2048.jpg)
![Spiritual development (Fowler)
[Intuitive projective]
Imitates religious behavior such as bowing
the head in prayer, but does not understand
the meaning.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-66-2048.jpg)
![Intellectual development (Jean Piaget)
[Intuitive phase] (4-7 yrs)
Children can repeat the event in play that occurred many
hours or day before.
Unable to accomplish true inductive or deductive reasoning.
Believes that all objects in the environment are there to
satisfy the human needs.
Oral development:
[Pre conventional morality] – Strictly for the purpose of self
interest that to avoid punishment and to have favors
turned.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-67-2048.jpg)
![Play (New Hall)
[Co-operative play] – Children begins to
exchange ideas with other children and
gradually interact in play activities.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-69-2048.jpg)
![Psychosocial development (Erick Erickson)
[Sense of industryVs Inferiority]
Industry- The people who are involved in
providing a service.
Inferiority- A state of feeling less important.
Engage in task in real world
Highly motivate in purposeful activity, Eg: include
them in planning menu. Encourage the child to
identify his potentials.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-80-2048.jpg)
![Psycho sexual (Freud)
[Latent phase]
Associate with same sex
Peers ignore the opposite sex](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-81-2048.jpg)
![Spiritual development (Fowler)
[Mythical literal faith]
Follows the rituals practiced in the family/society
Believes others, differentiate their thinking](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-82-2048.jpg)
![Intellectual development (Jean Piaget)
[Concrete operational stage]
Able to understand, read and write
Developing problem solving abilities
Asks questions](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-83-2048.jpg)
![Play (Newhall)
[Competitive play]
Girls:
Cooking
Grooming
Teaching
Boys:
Kites
Cycling
Team sports](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-85-2048.jpg)
![Psychosocial (Erick Erickson)
Early- [Identity Vs Role confusion]
Identity - Wrong person
Role confusion- Confusion in their own role
Who am I?
Intense loyalty to peer group
Begins to separate from parents
Later- [IntimacyVs Isolation]
Intimacy – Having close personal relationship with someone.
Isolation – Separate from others.
Develops intimacy with self and persons of both sexes.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-94-2048.jpg)
![Psycho sexual (Freud)
[Genital stage] – Masturbation and sexual
fantasies are common](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-95-2048.jpg)
![Spiritual development (Fowler)
[Conventional faith]
Personal and social values evolved to support
their identity to explore religious affiliation.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-96-2048.jpg)
![Intellectual development (Jean Piaget)
[Formal operational stage]
Thinking is oriented to things and events that
they can observe directly.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-97-2048.jpg)
![Moral development (Kohl berg)
[Post conventional stage]
Able to differentiate from right and wrong.](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-98-2048.jpg)
![Play (Newhall)
[Social play]
Sports
Parties
Telephone conversations
WatchingTV
Computer game](https://image.slidesharecdn.com/growthanddevelopmentofallagegroups-171001102804/75/Growth-and-development-of-all-age-groups-Juhin-J-100-2048.jpg)
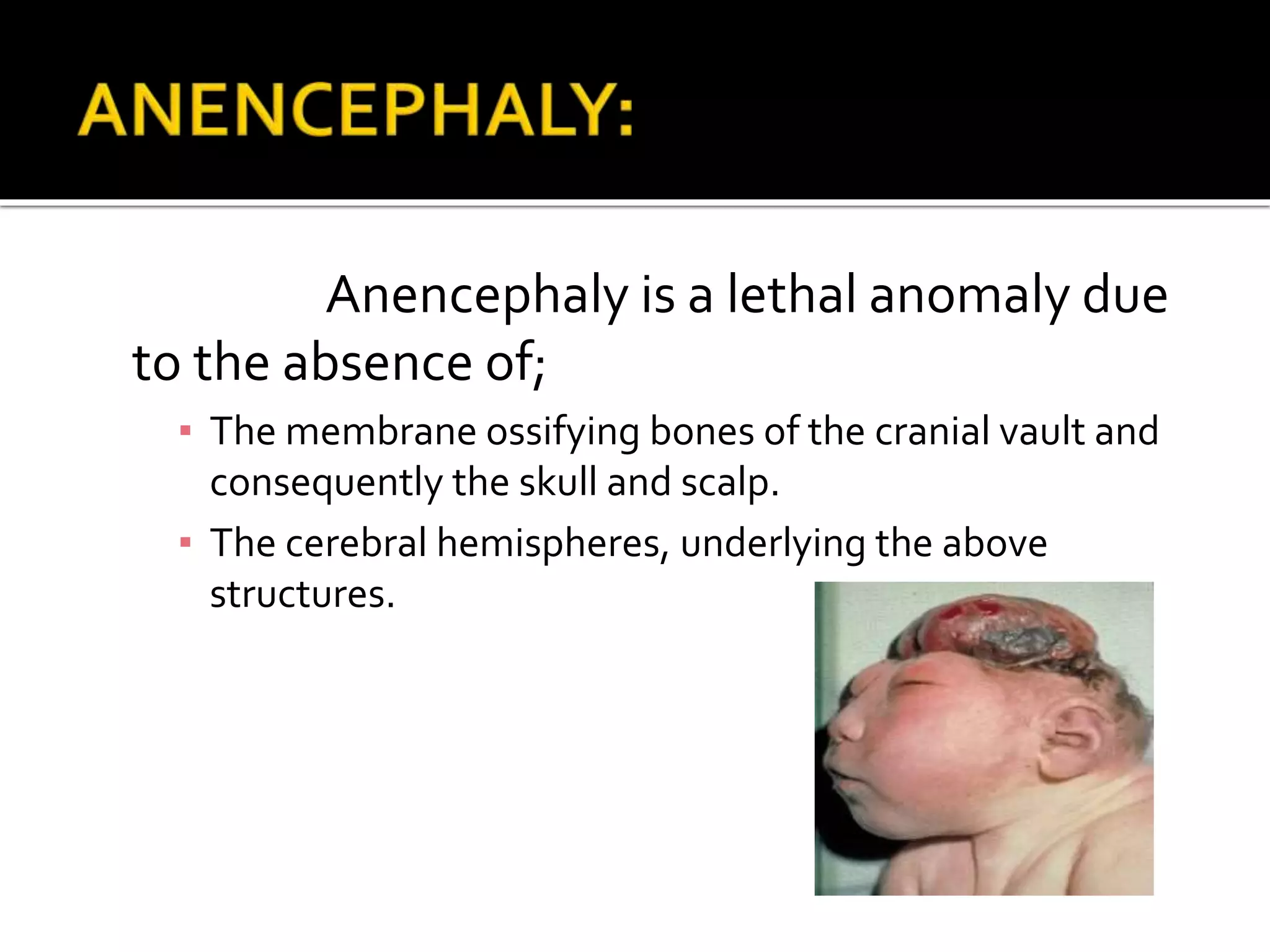
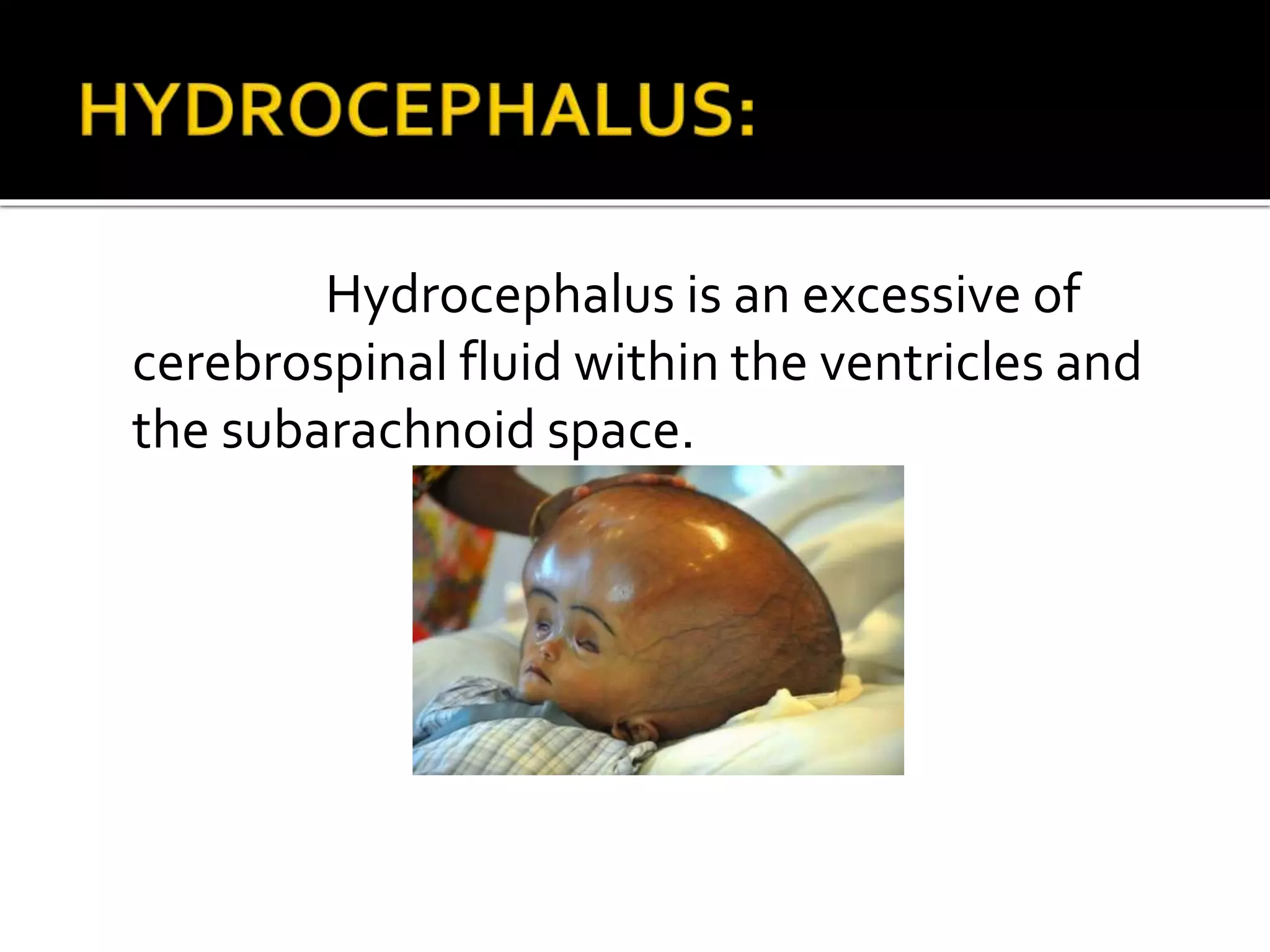
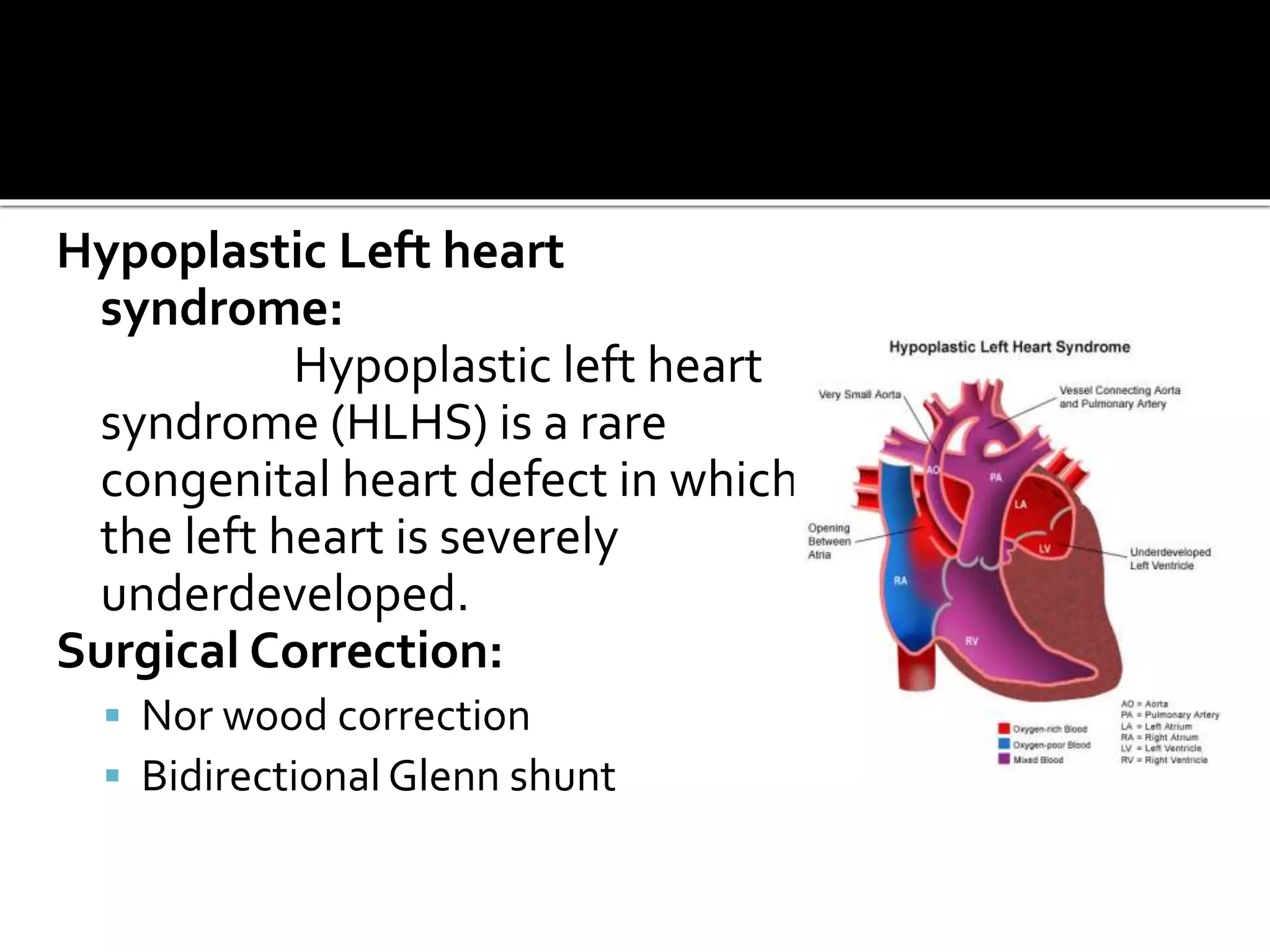
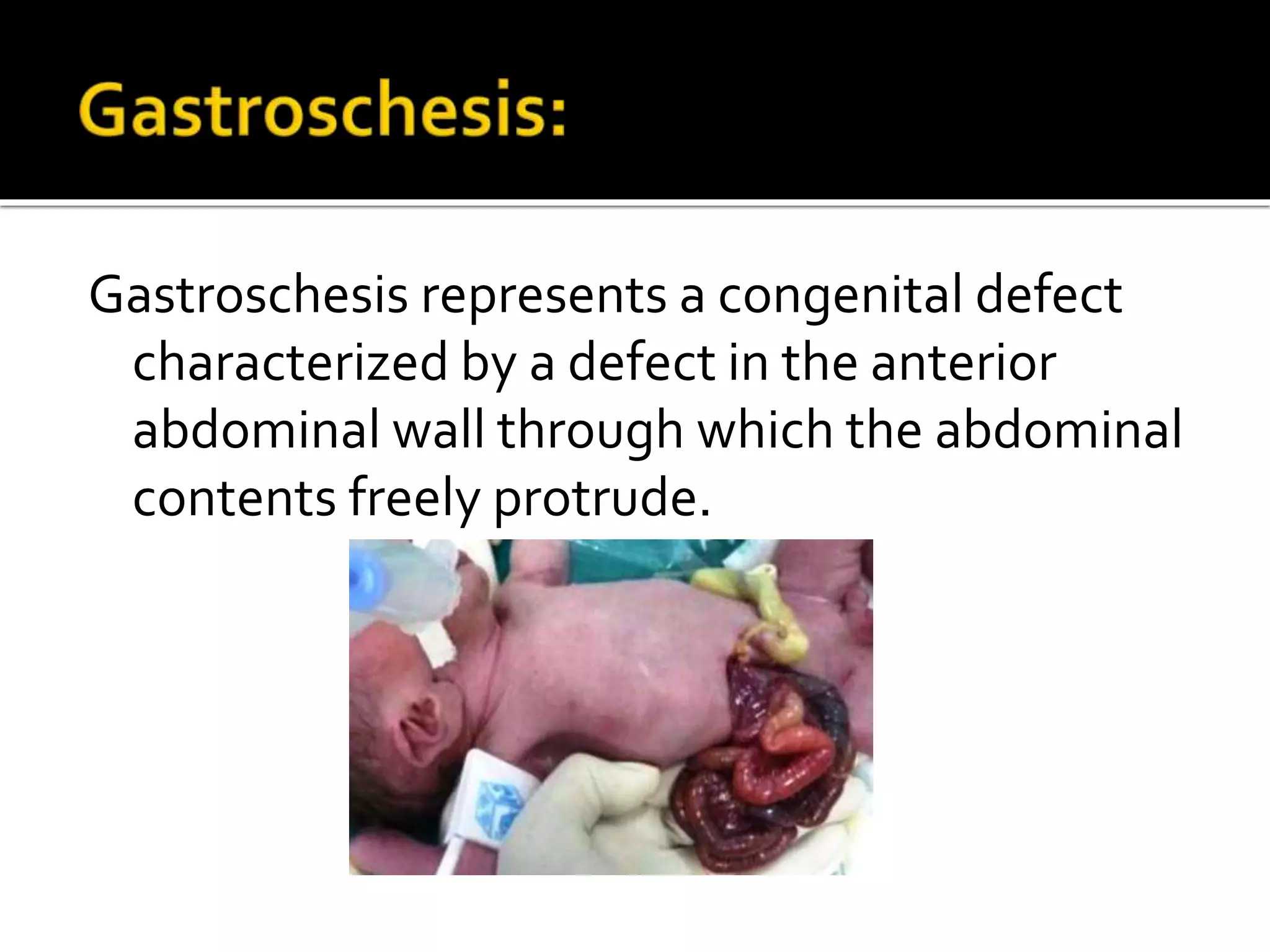
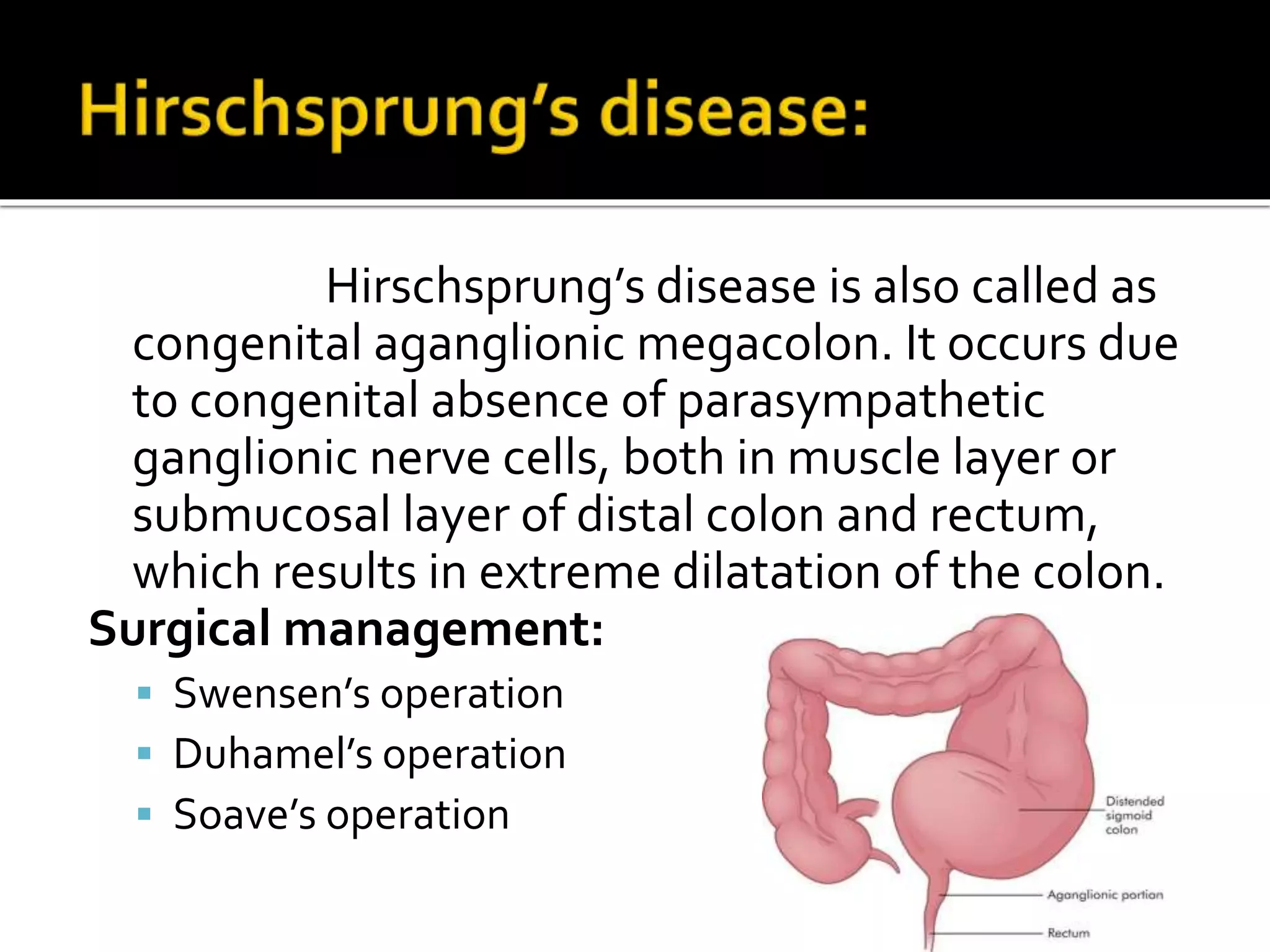
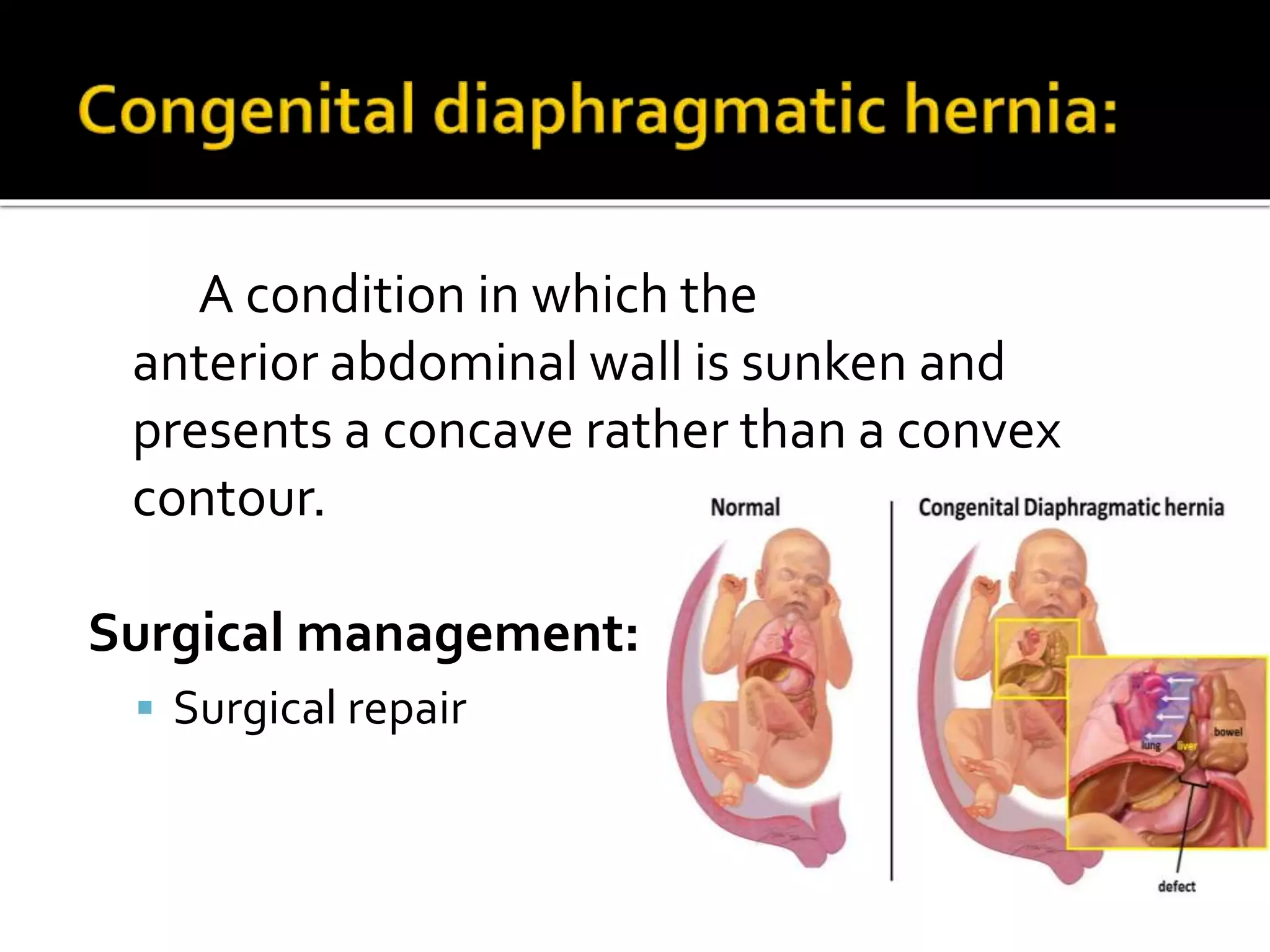
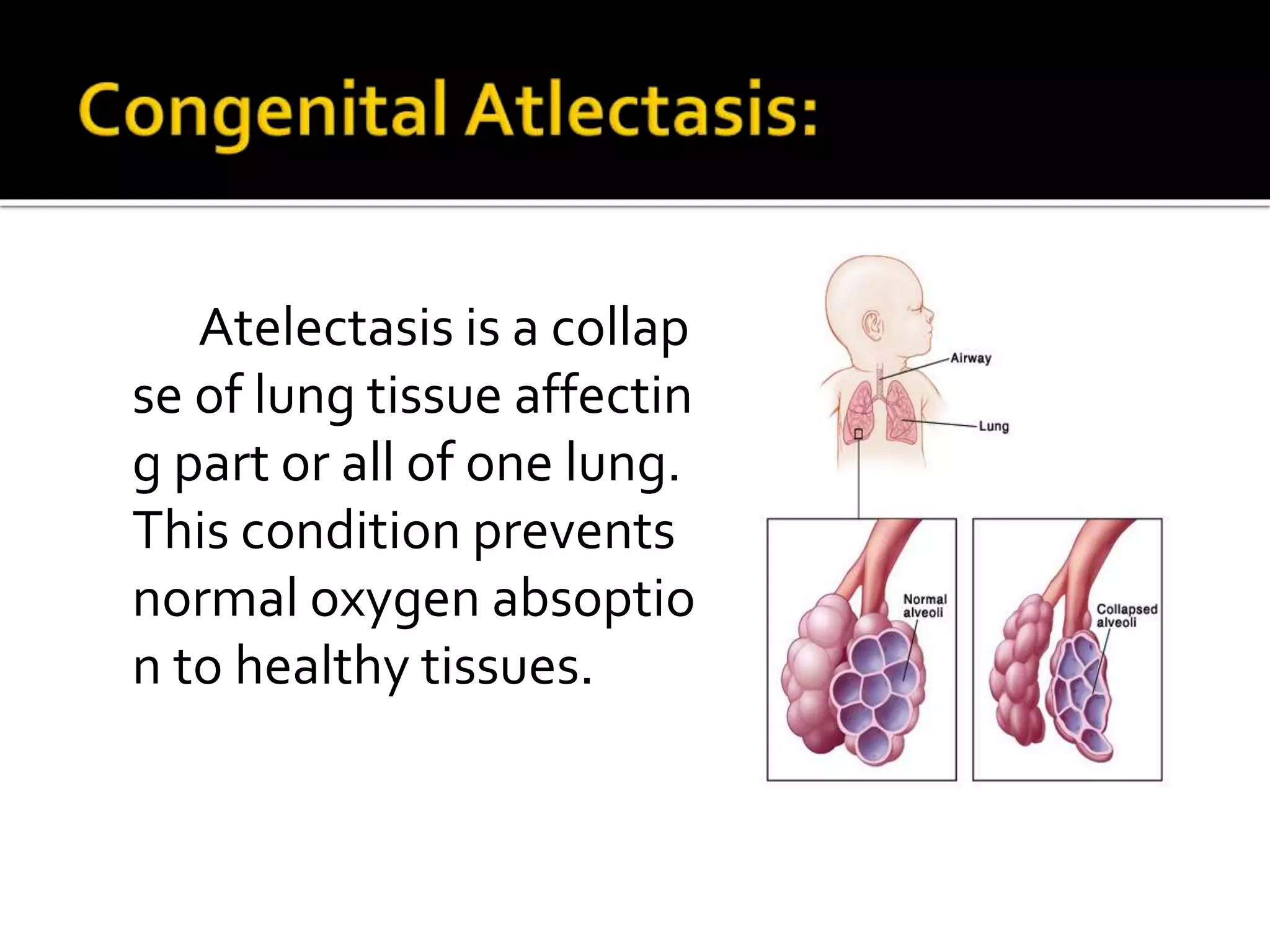
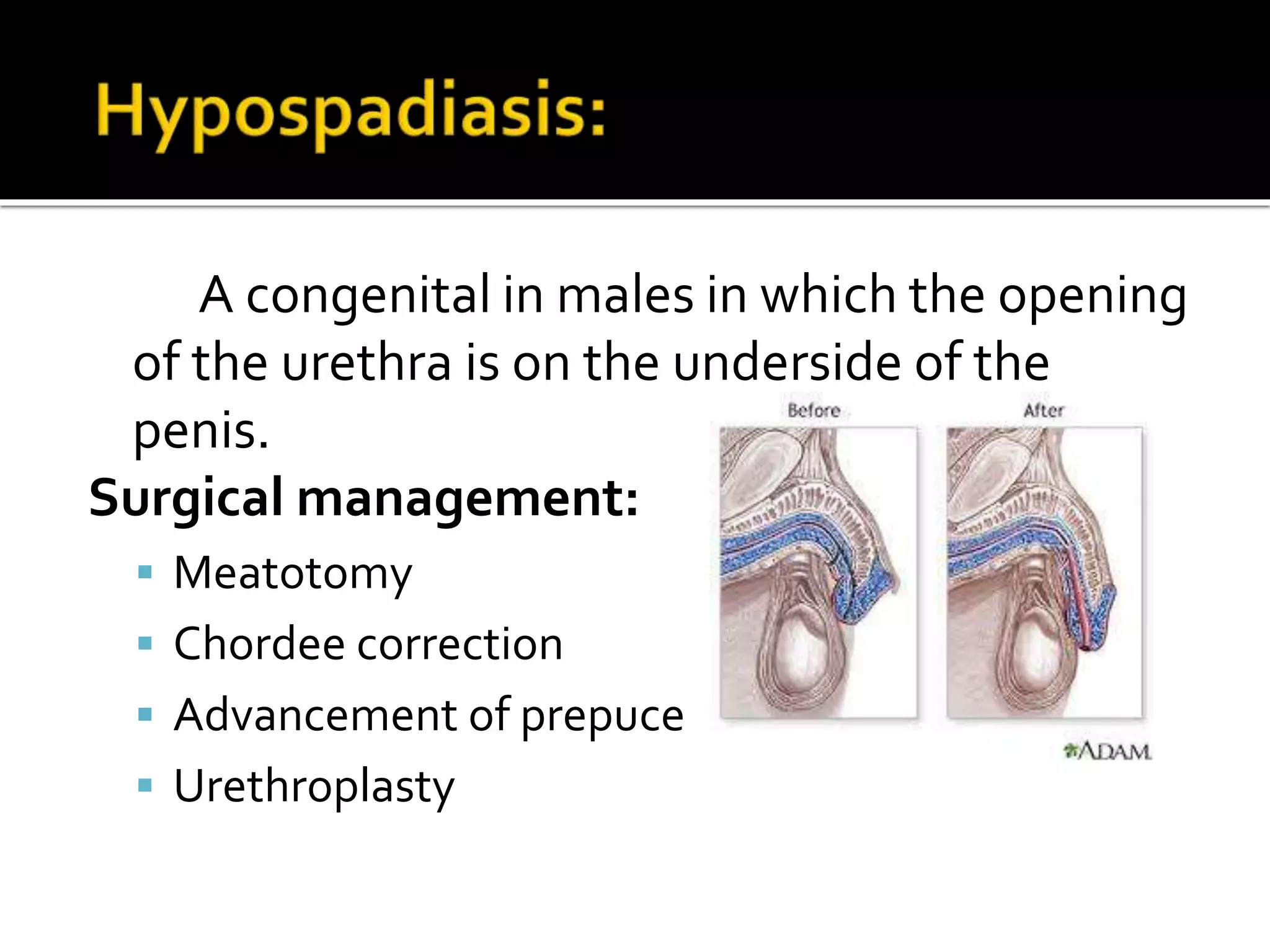
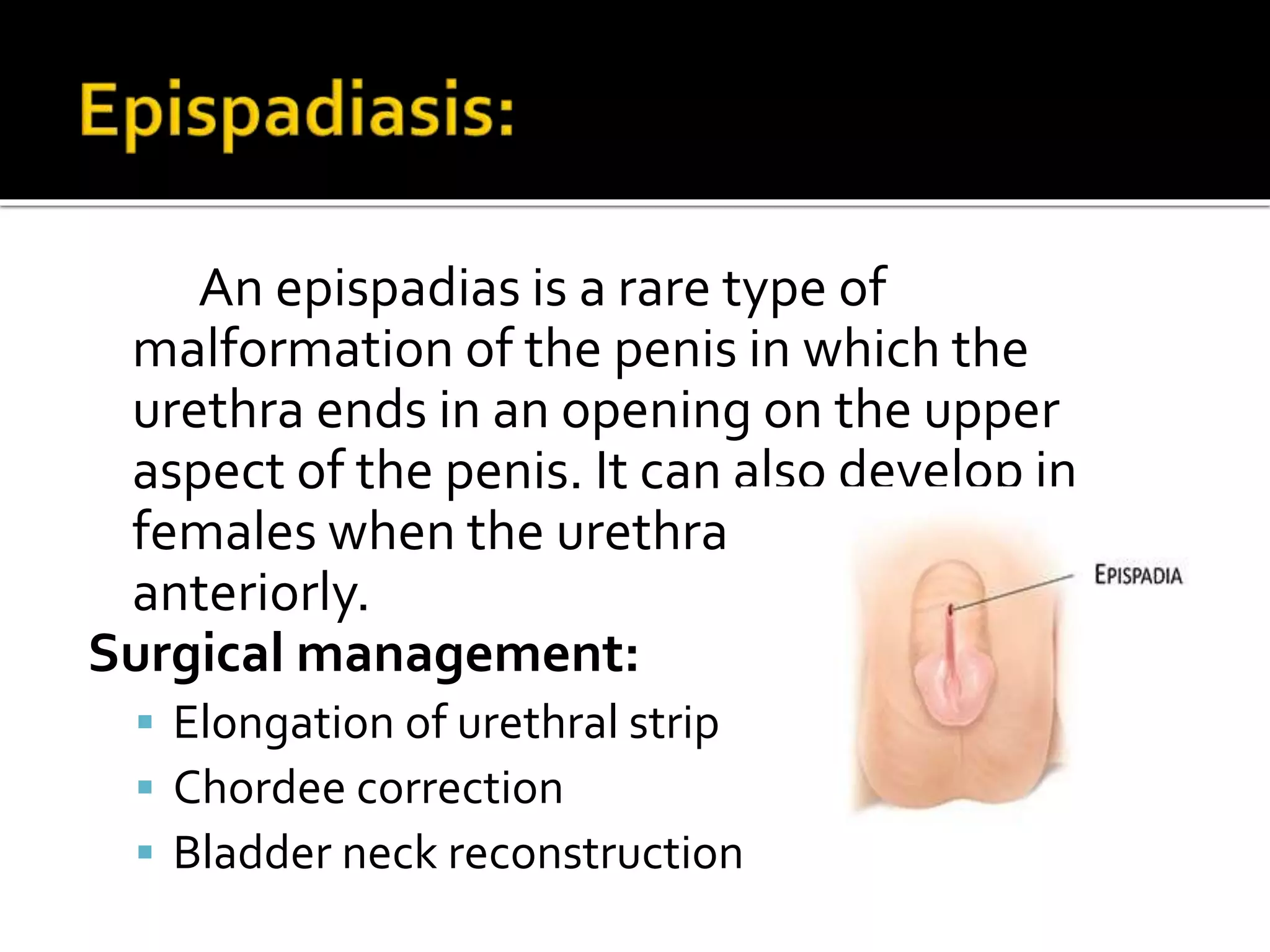
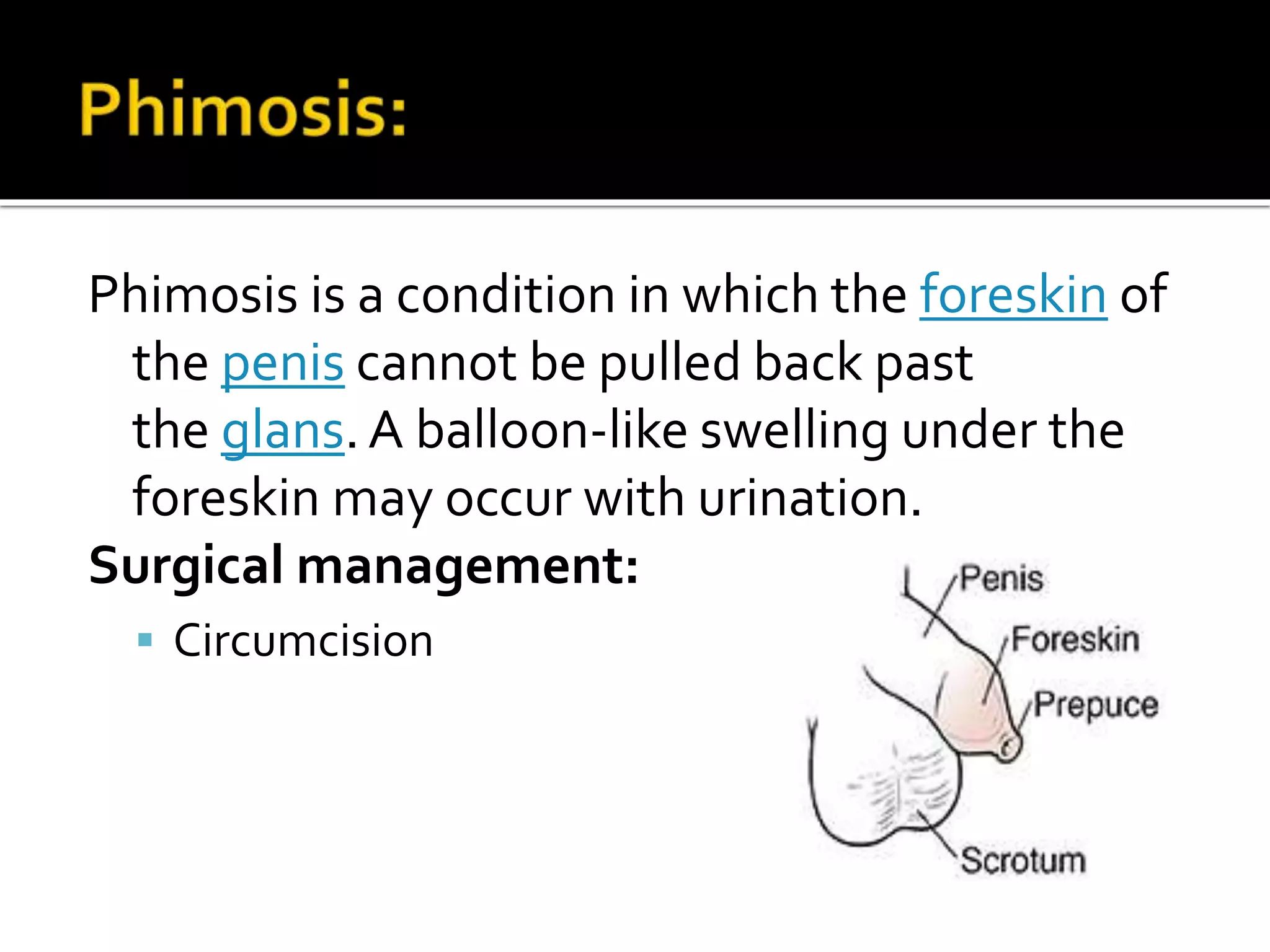
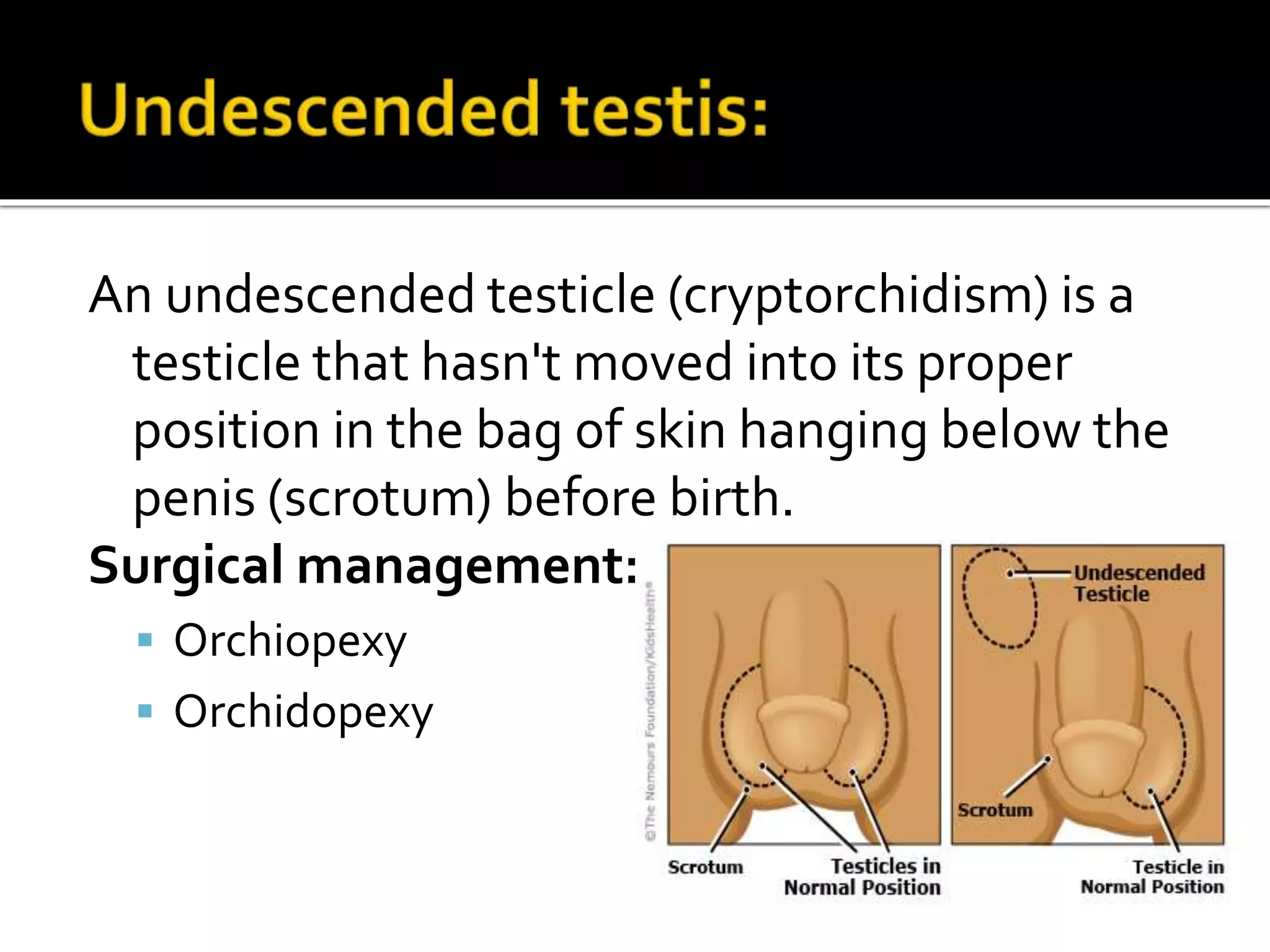
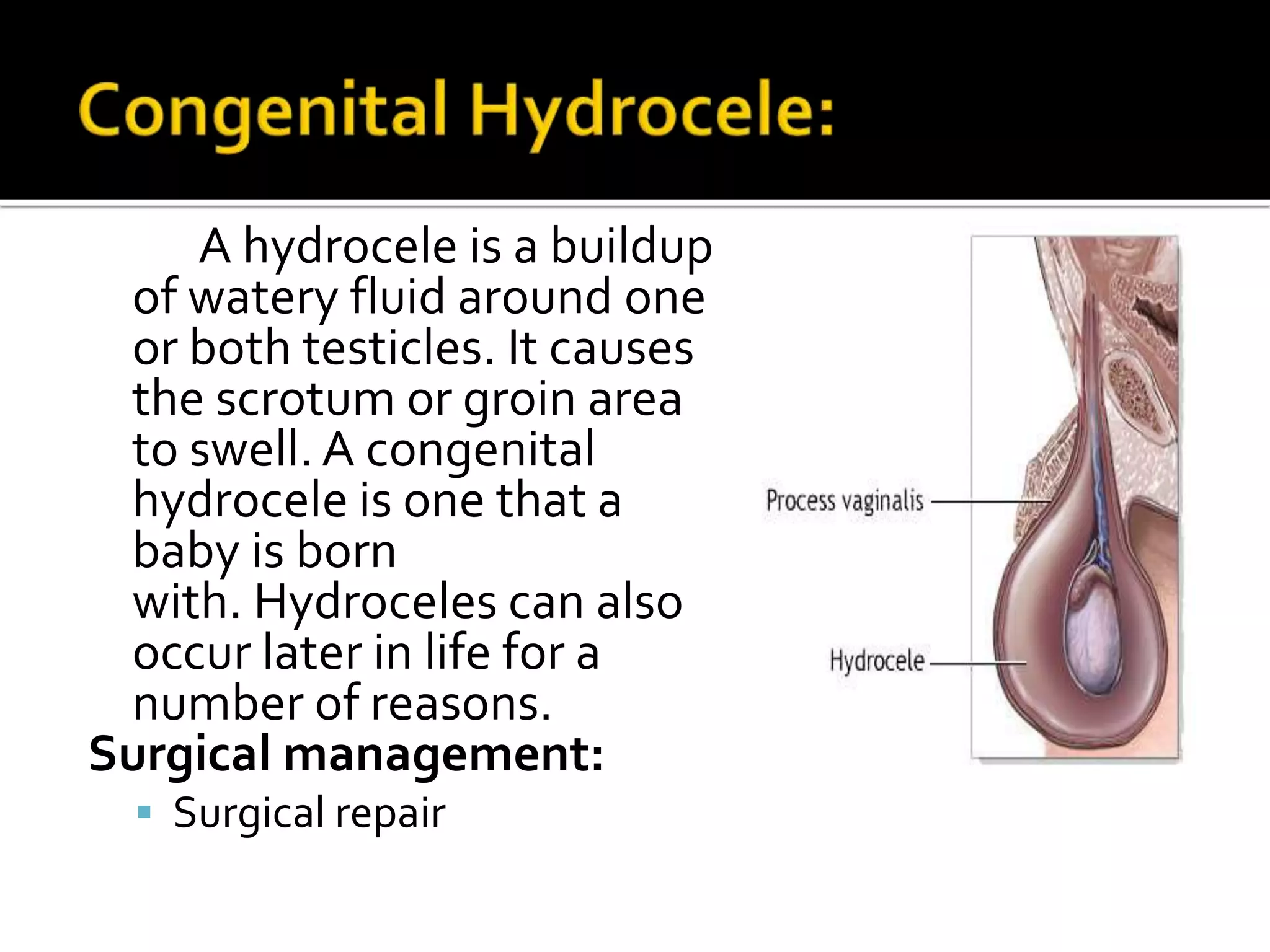
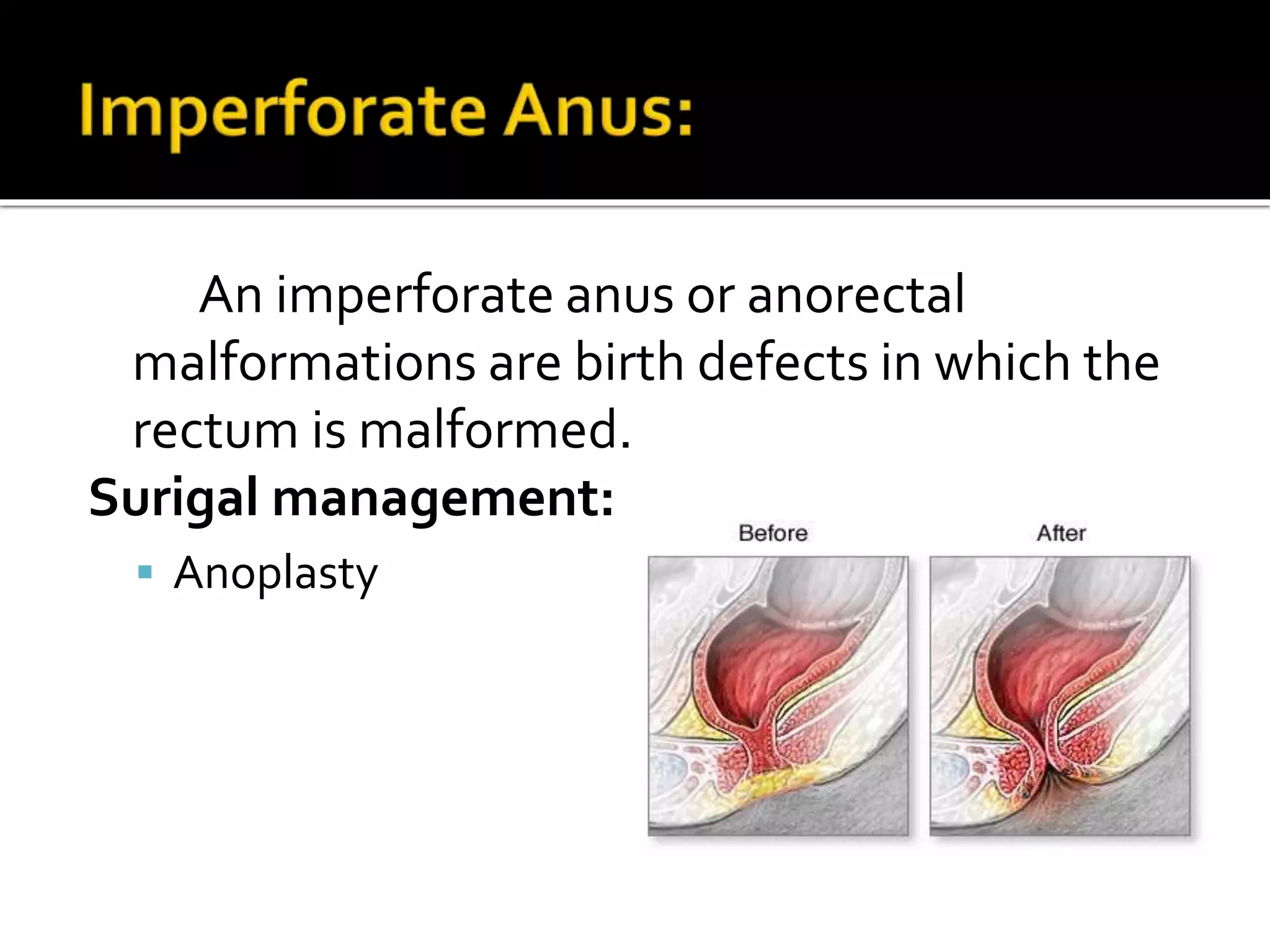
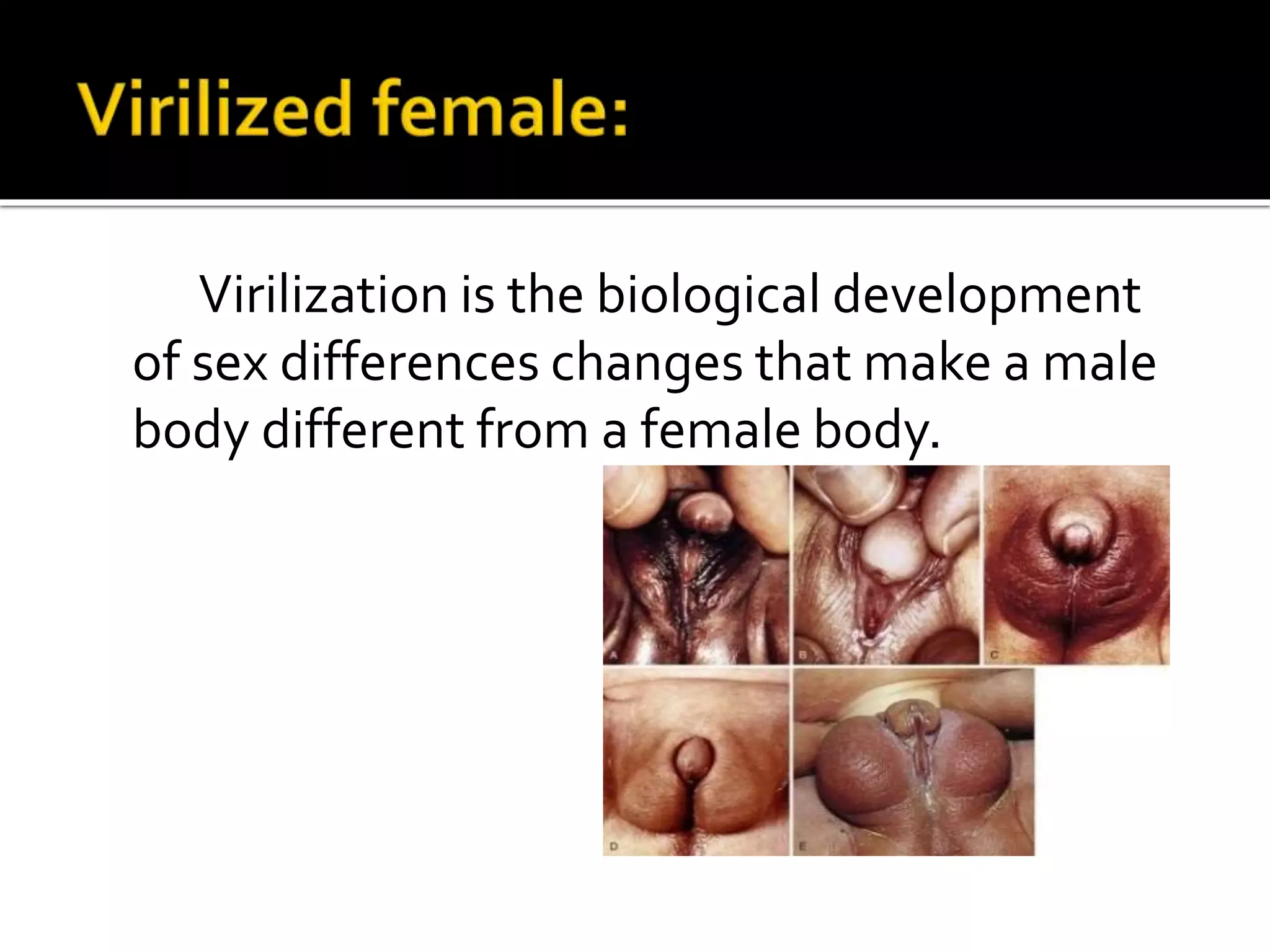
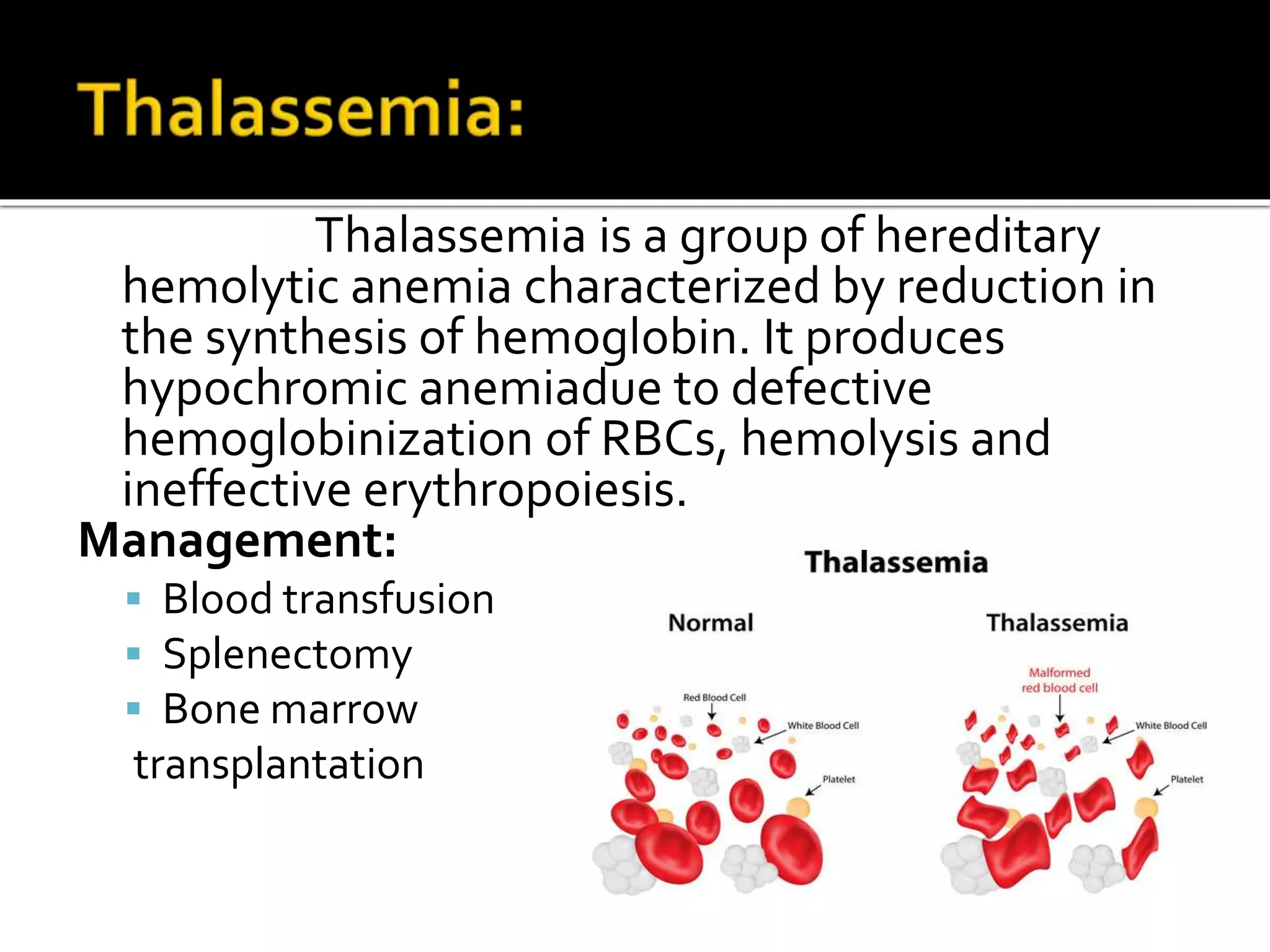
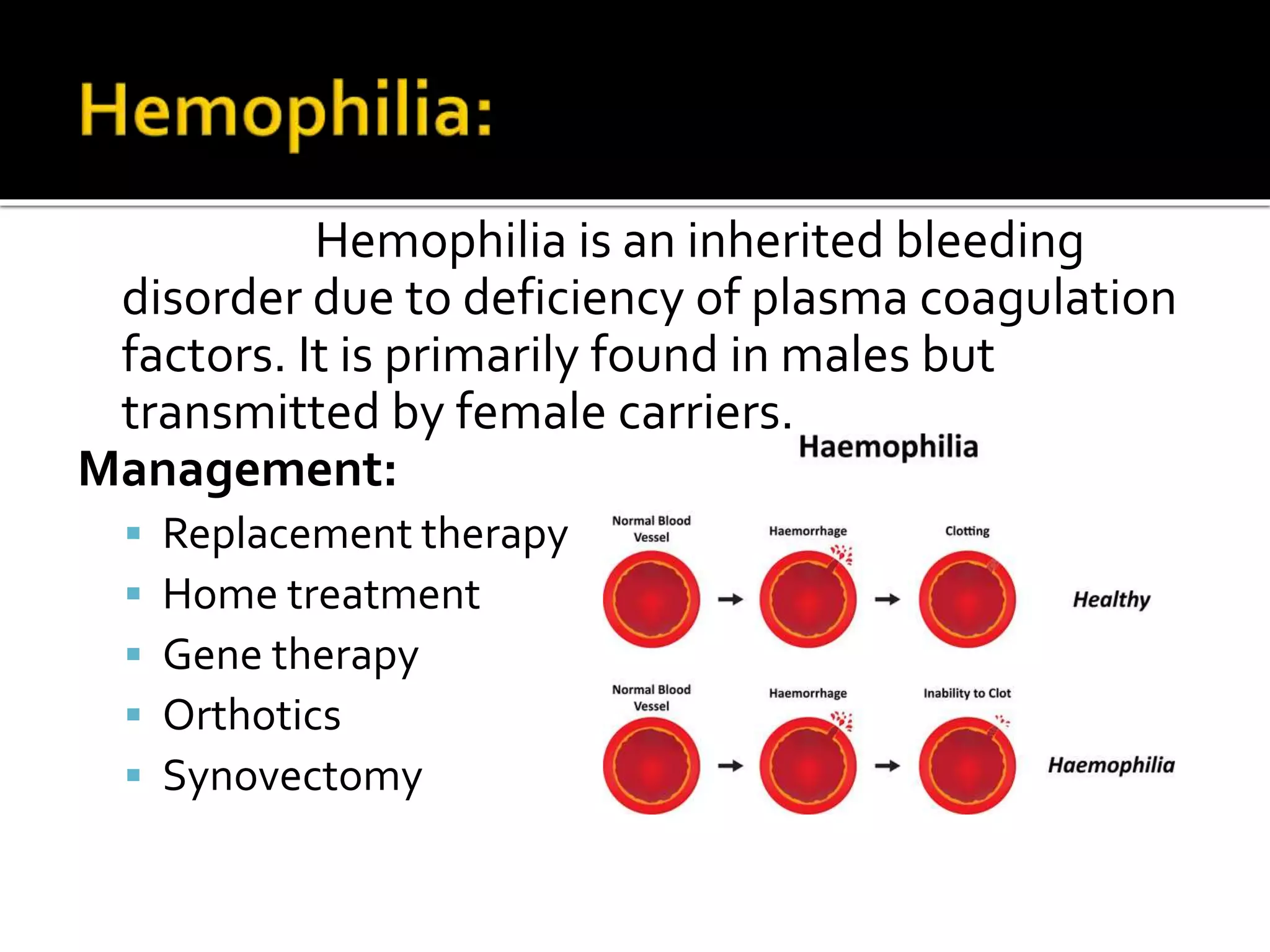
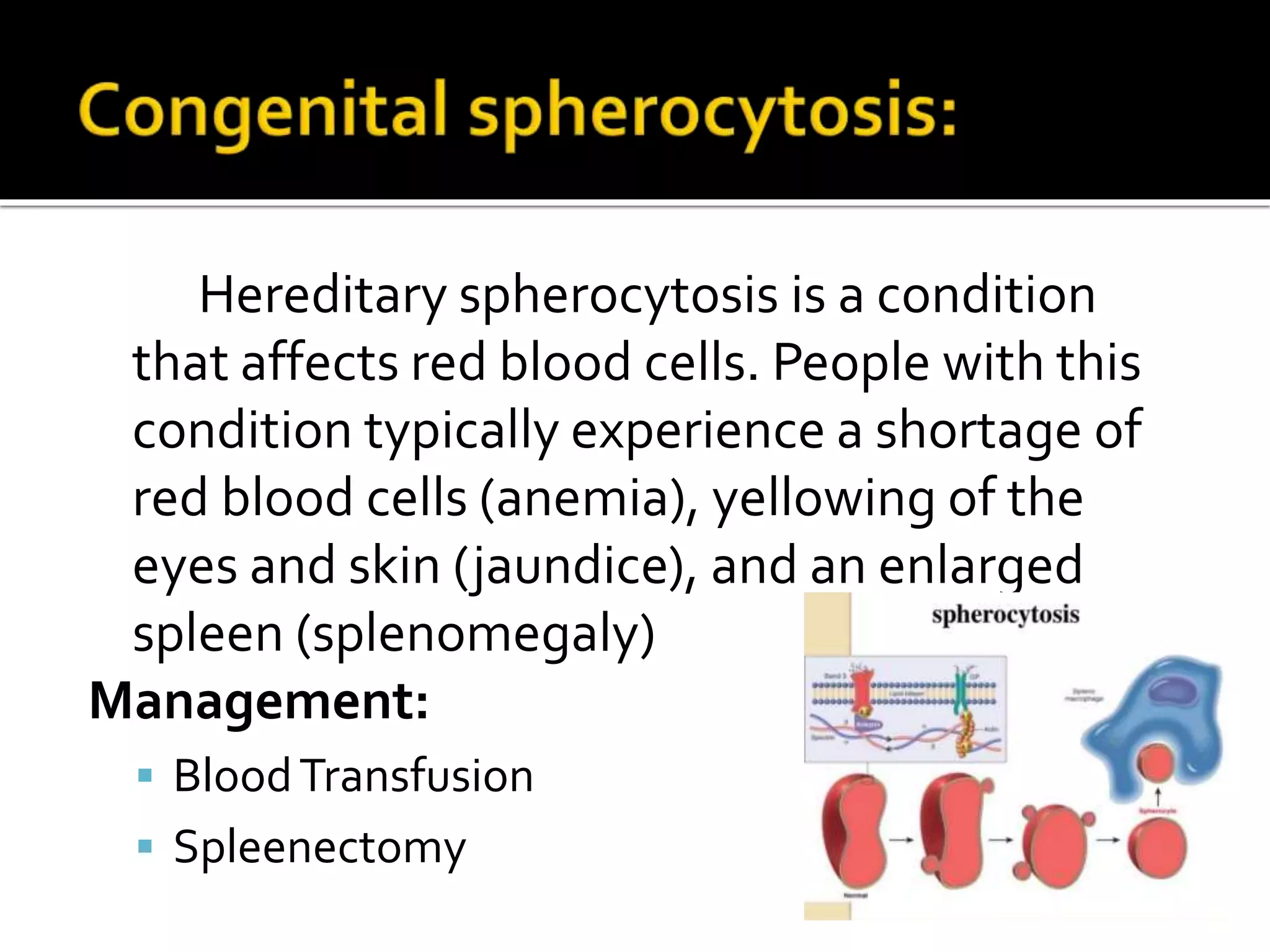
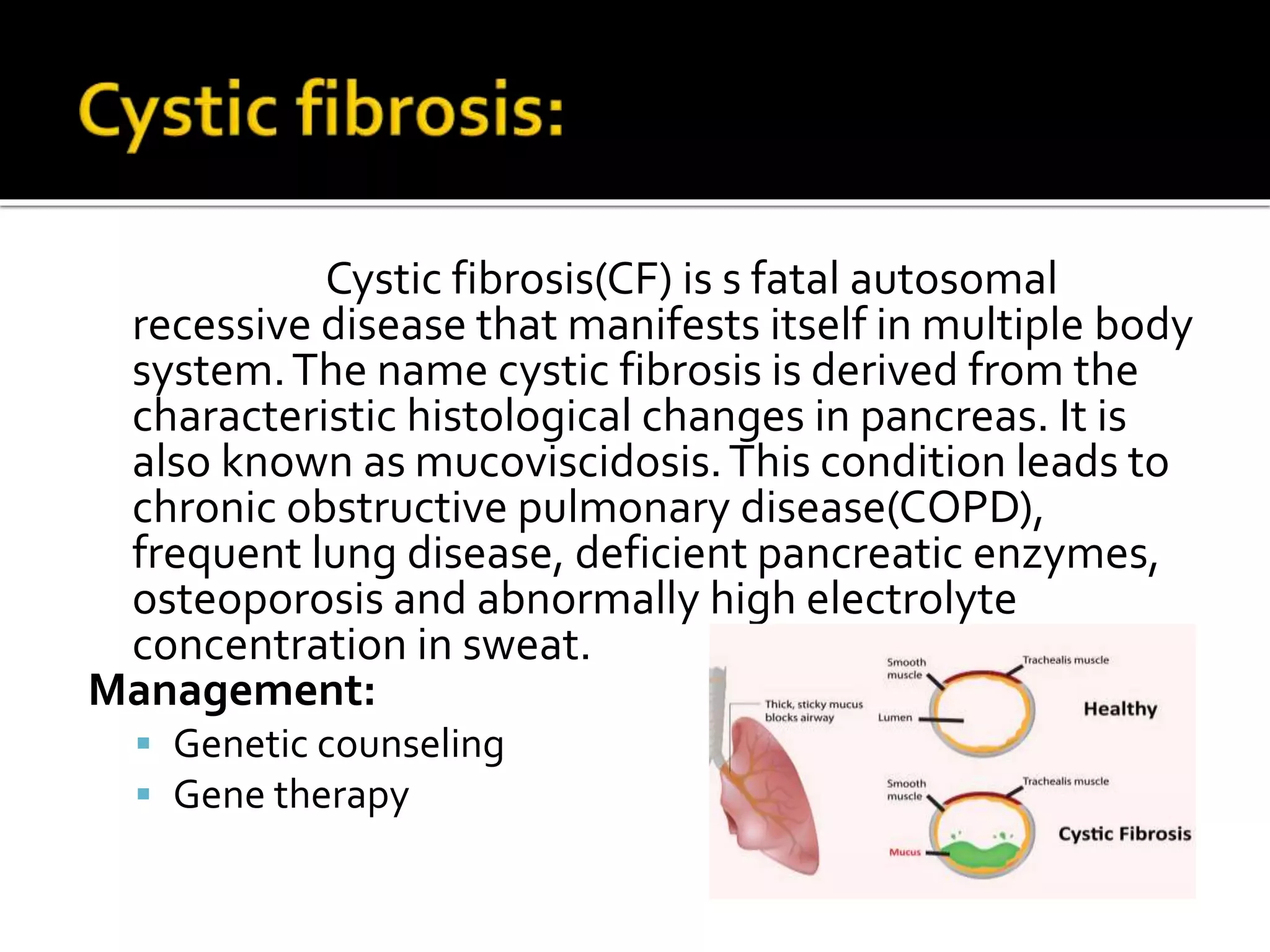
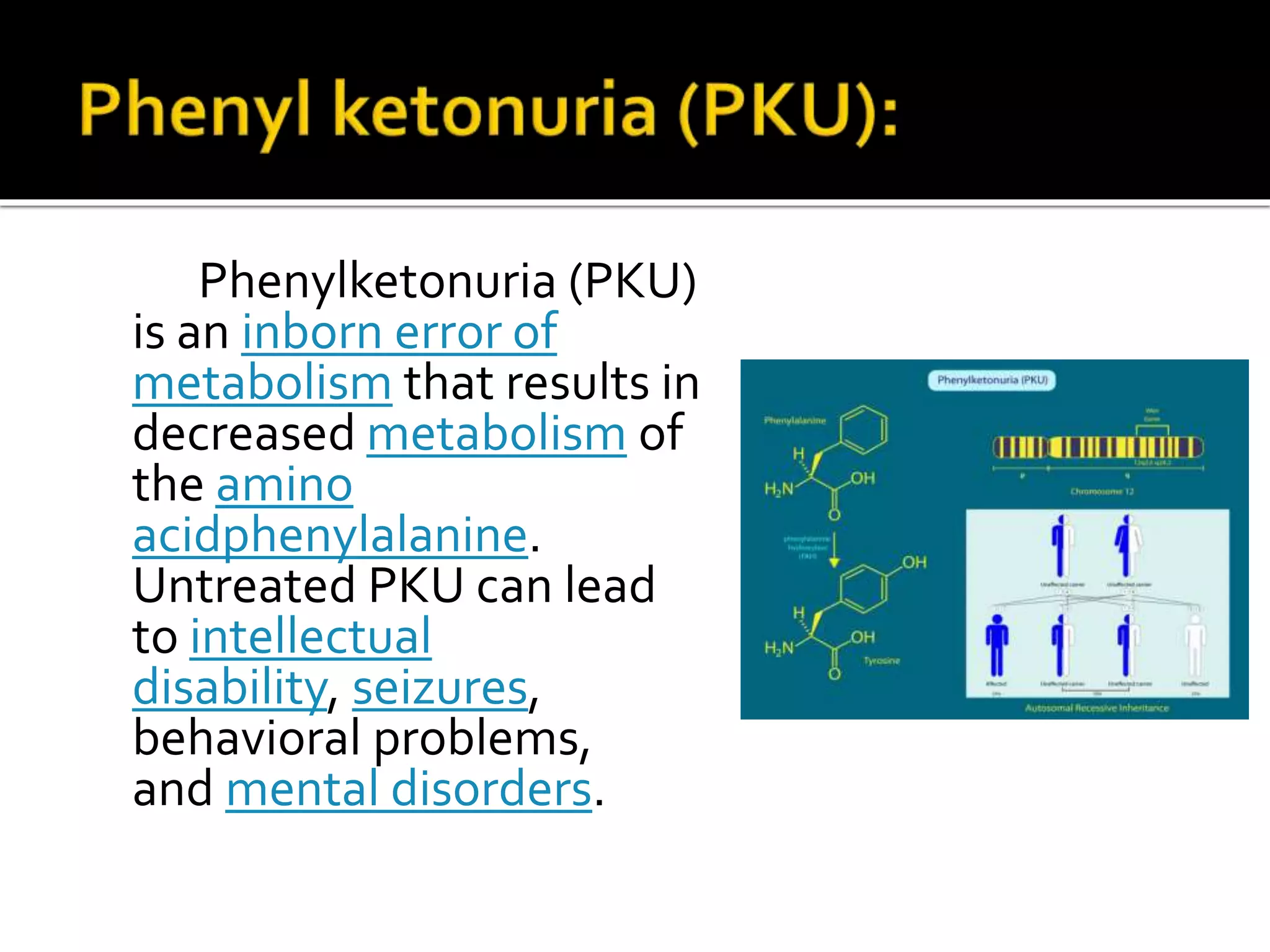
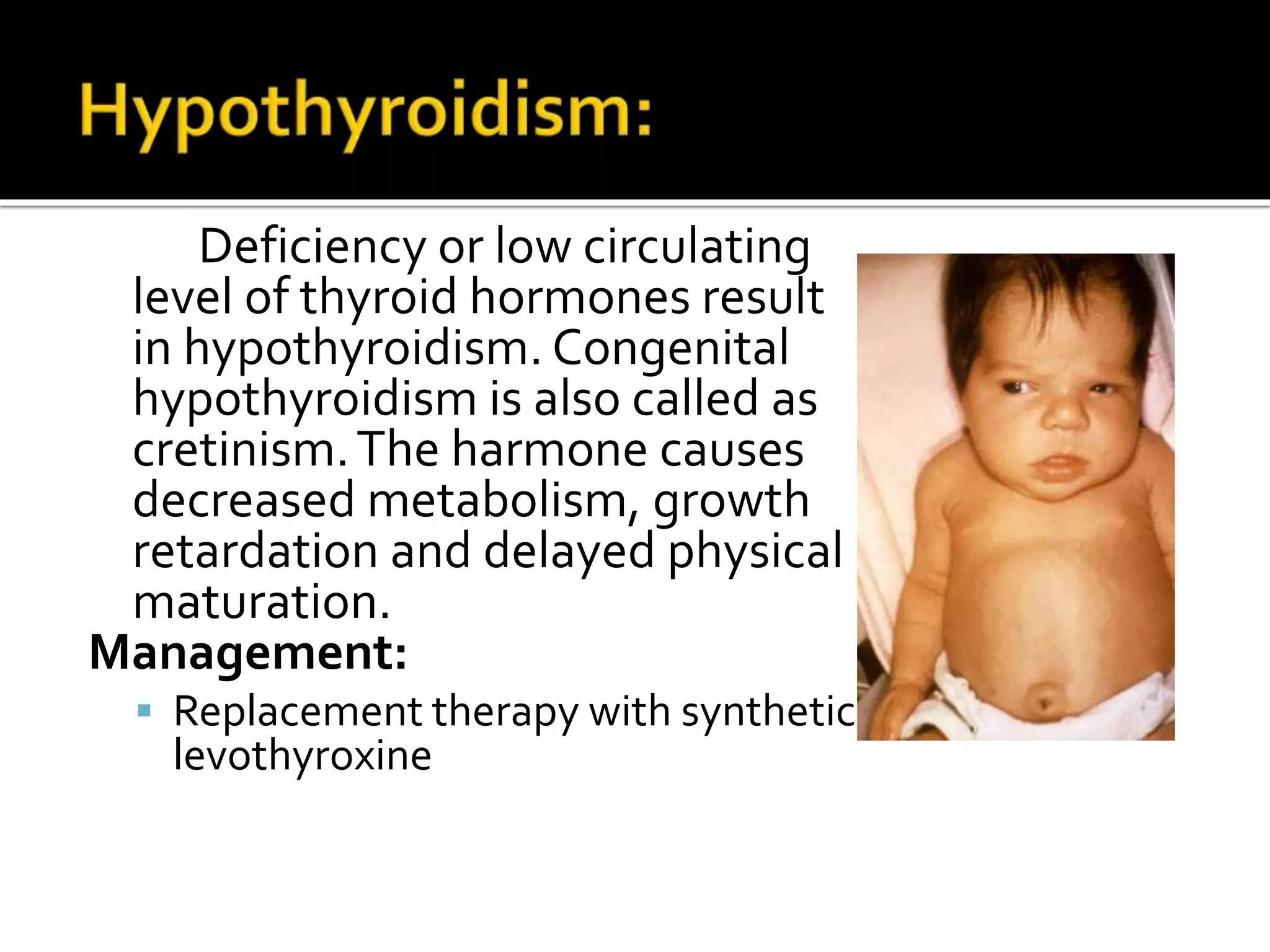
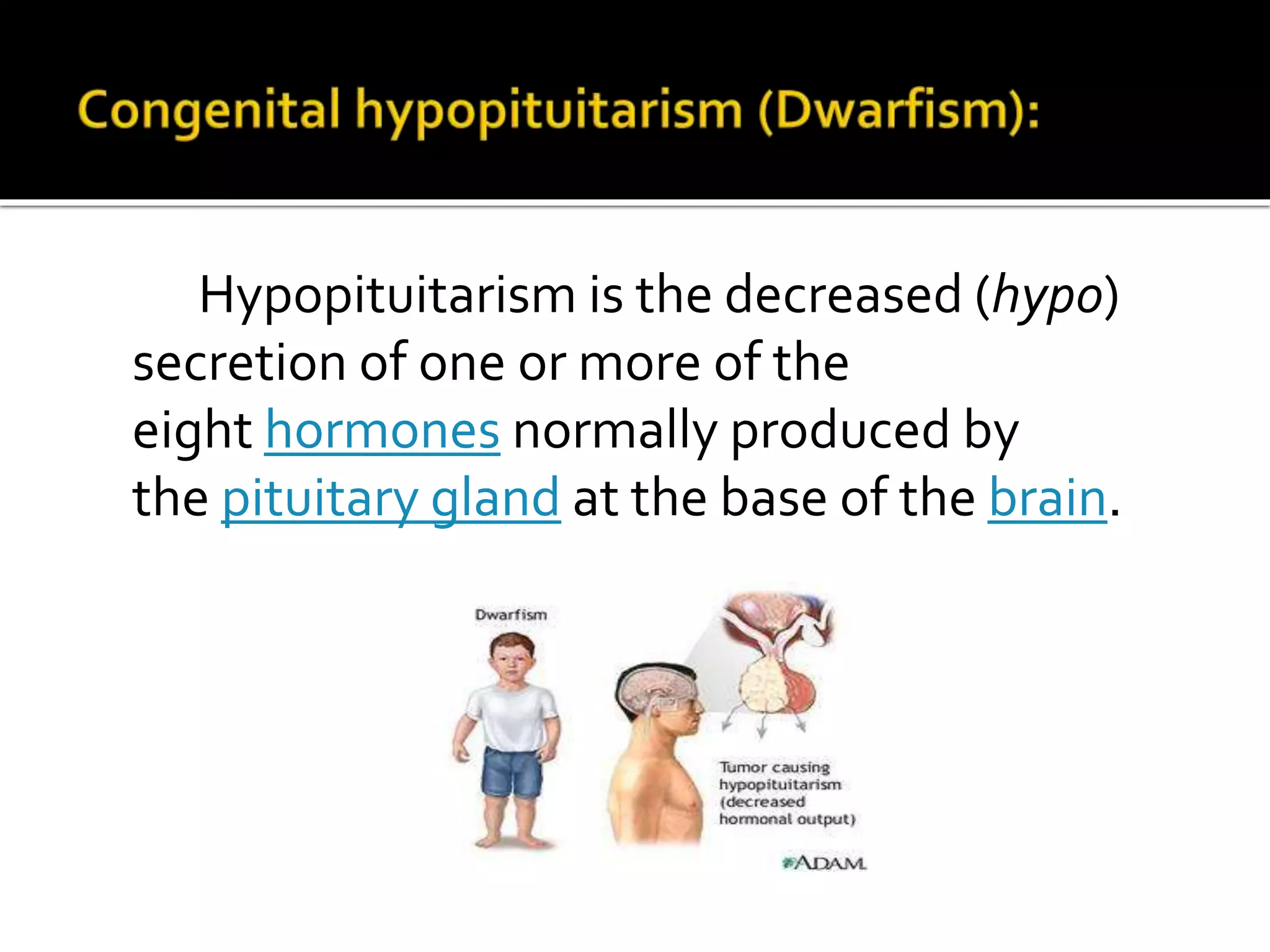
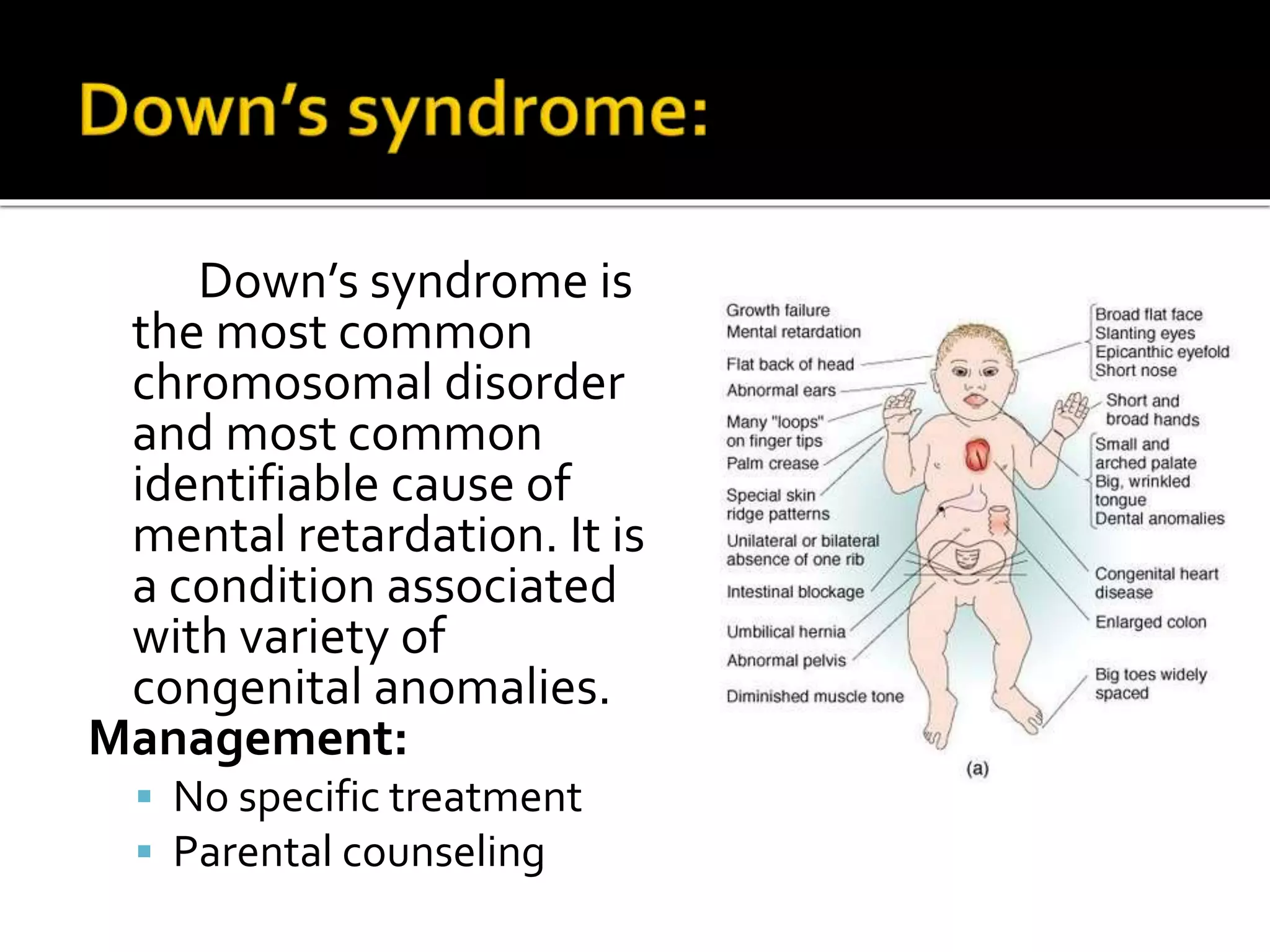
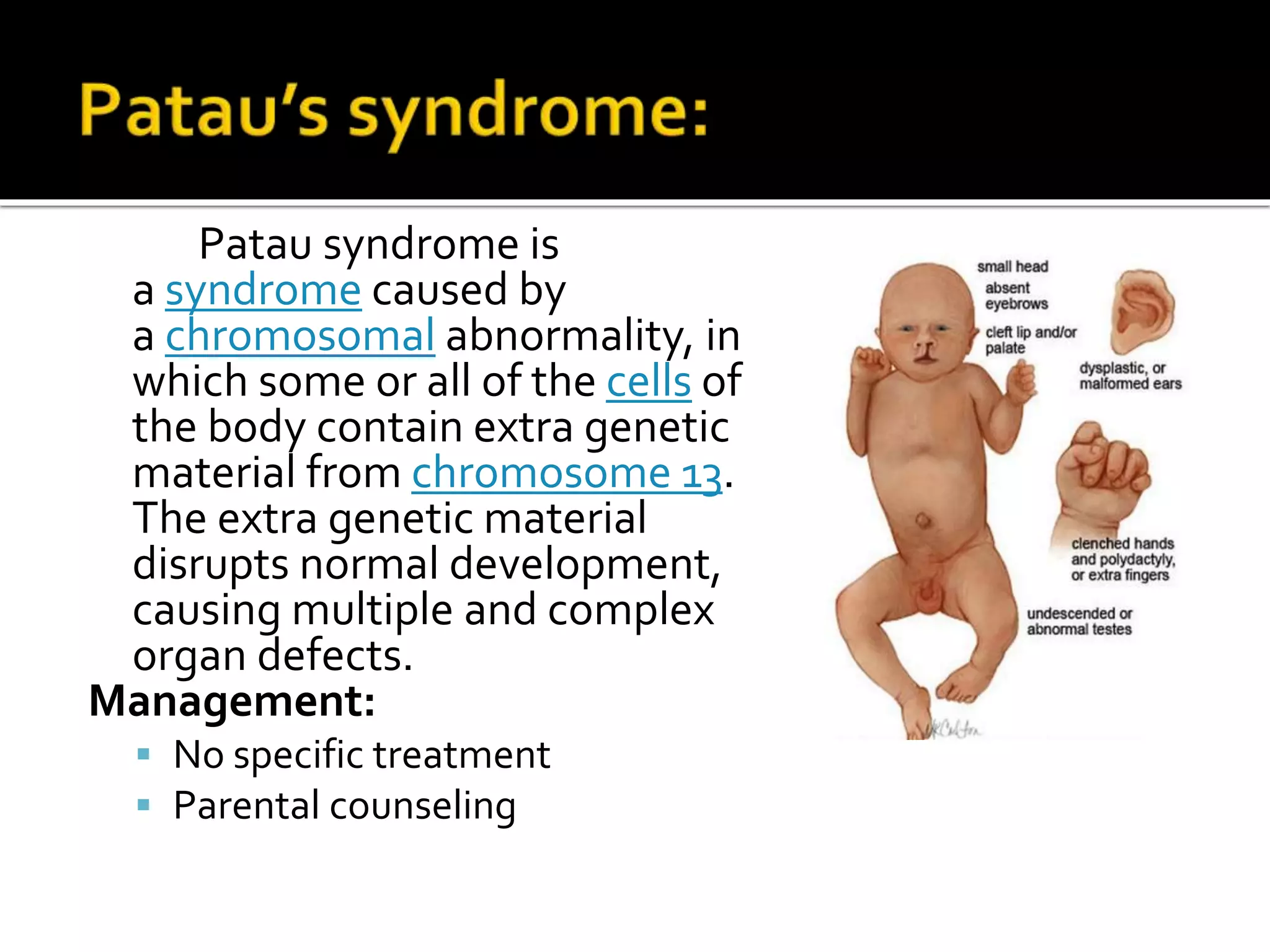
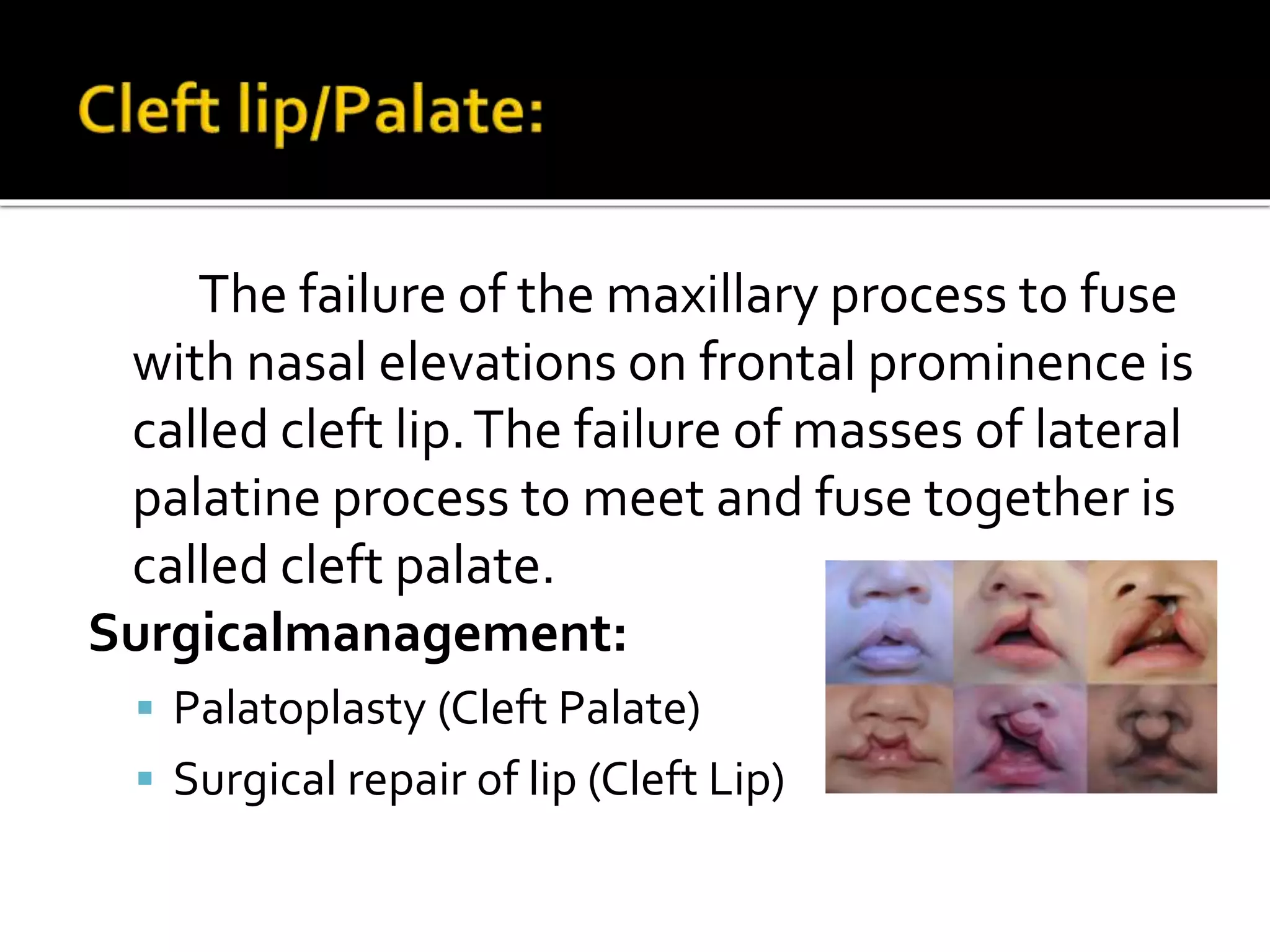


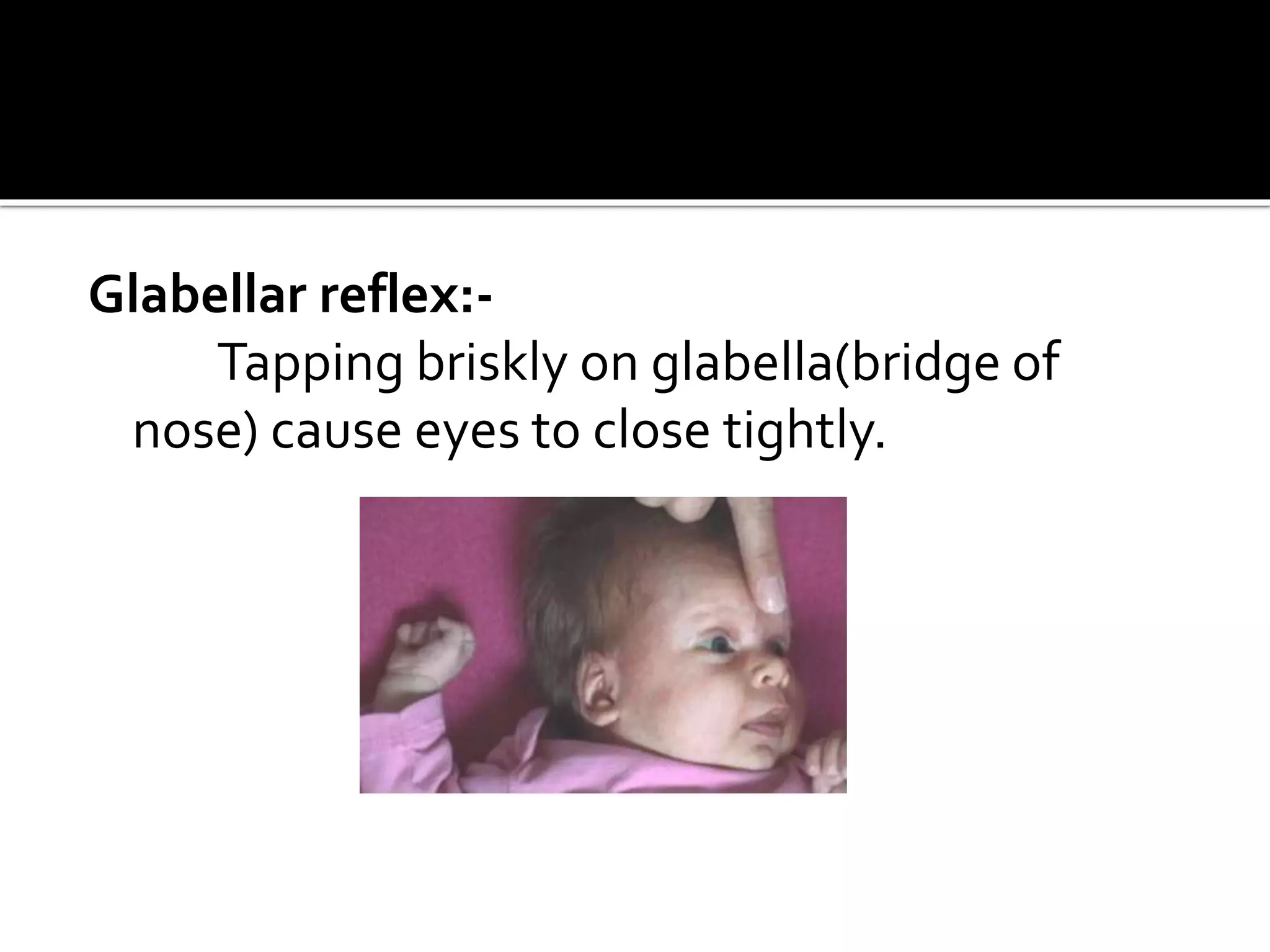
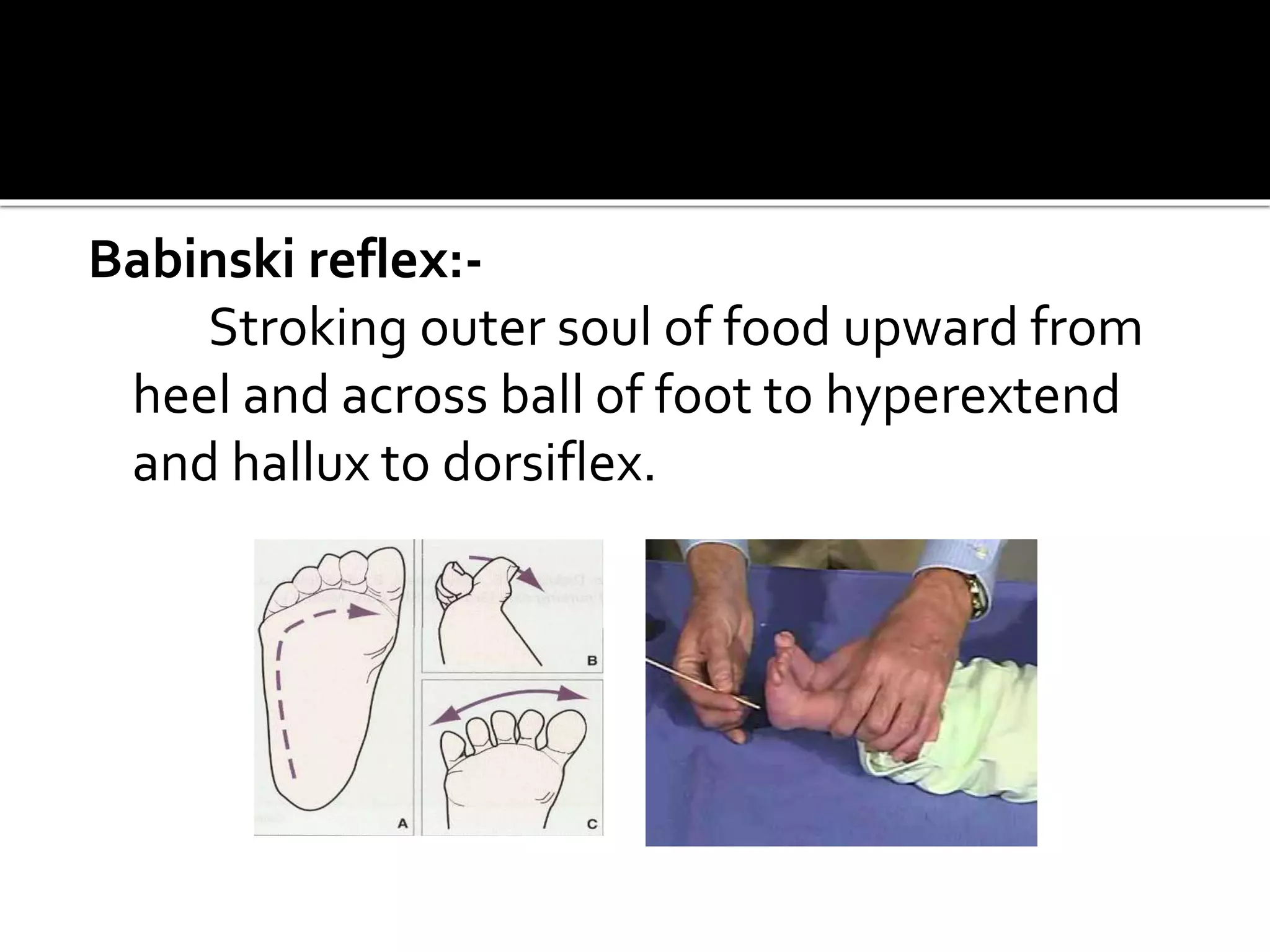
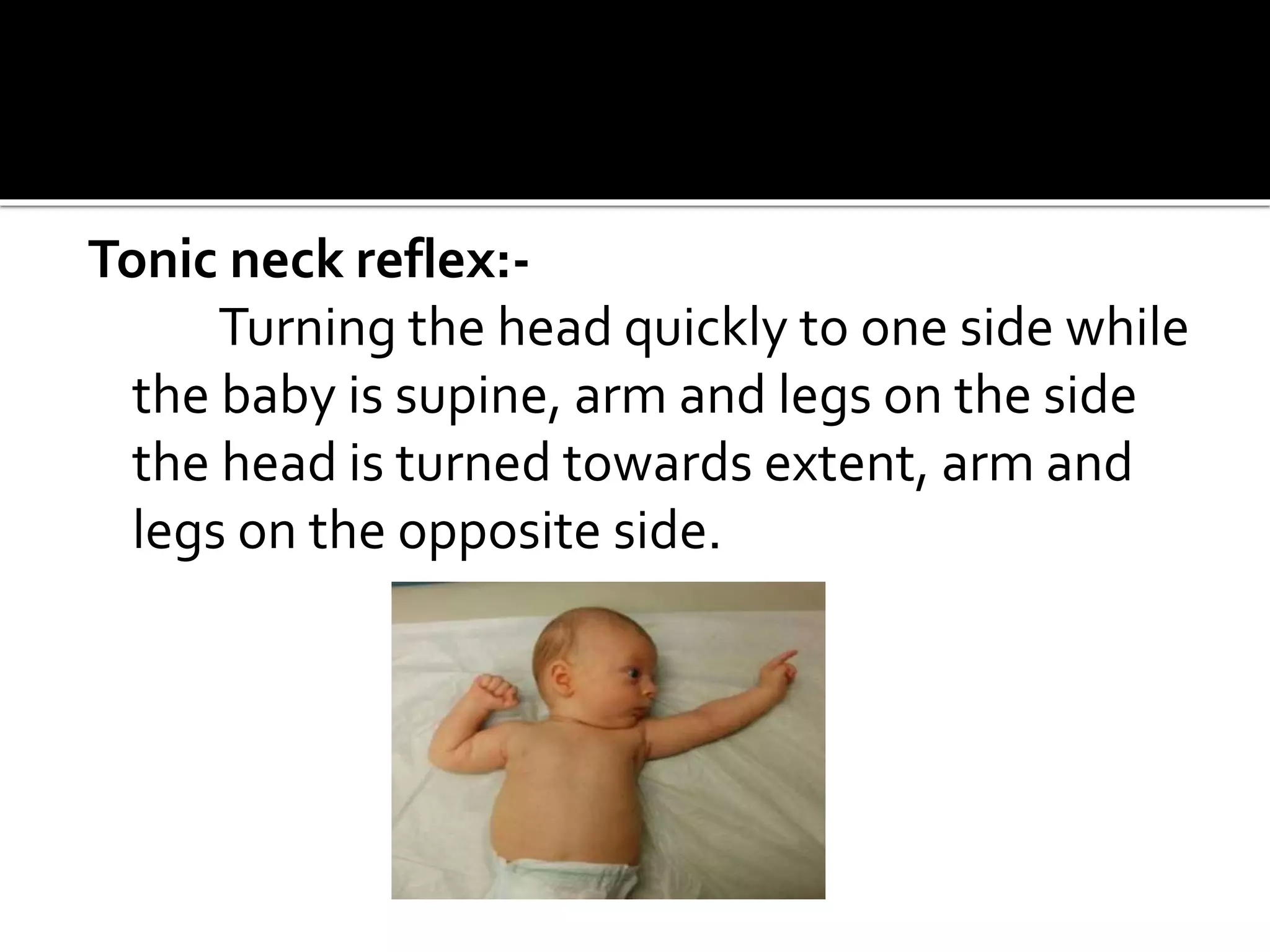
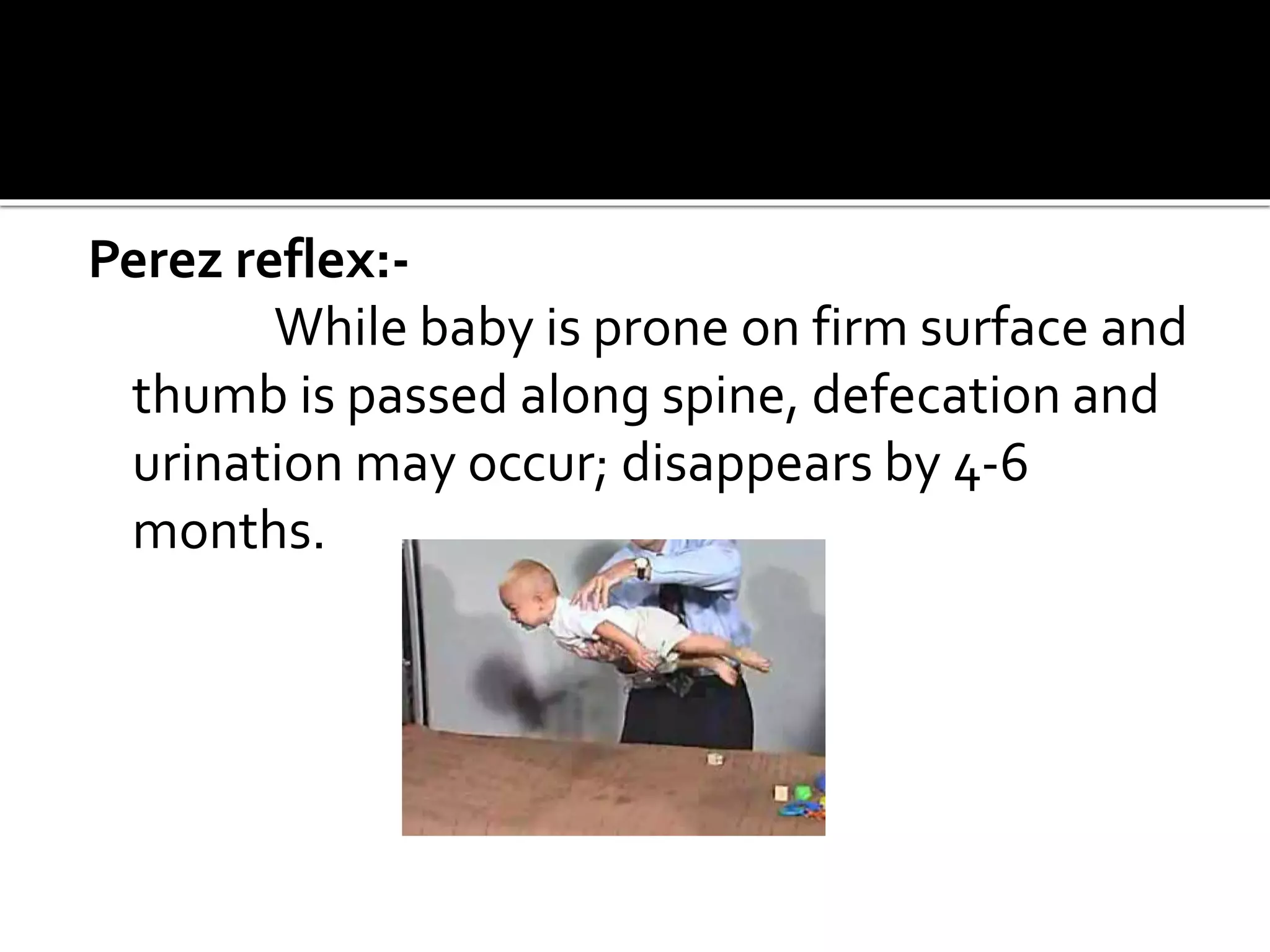
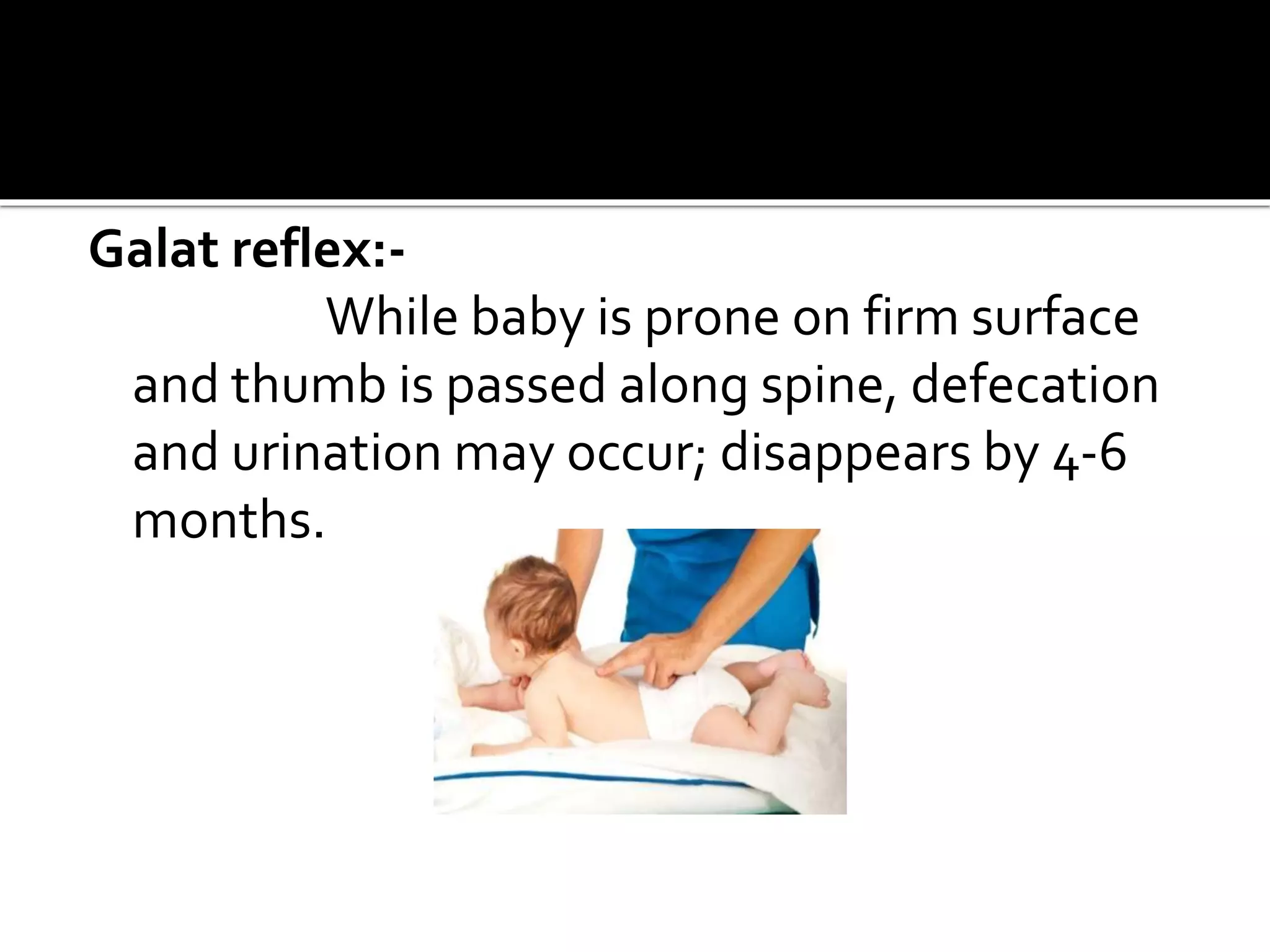
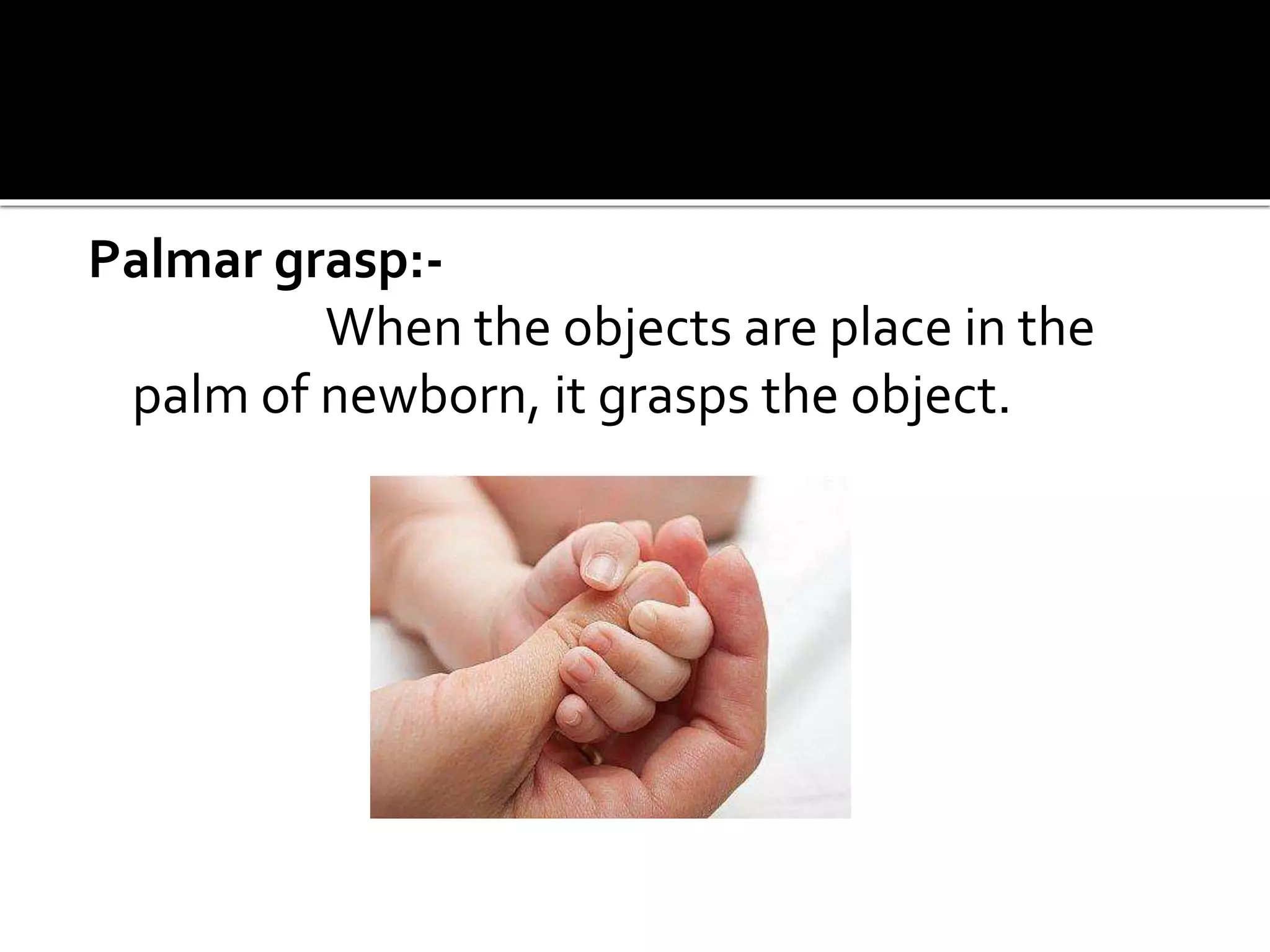
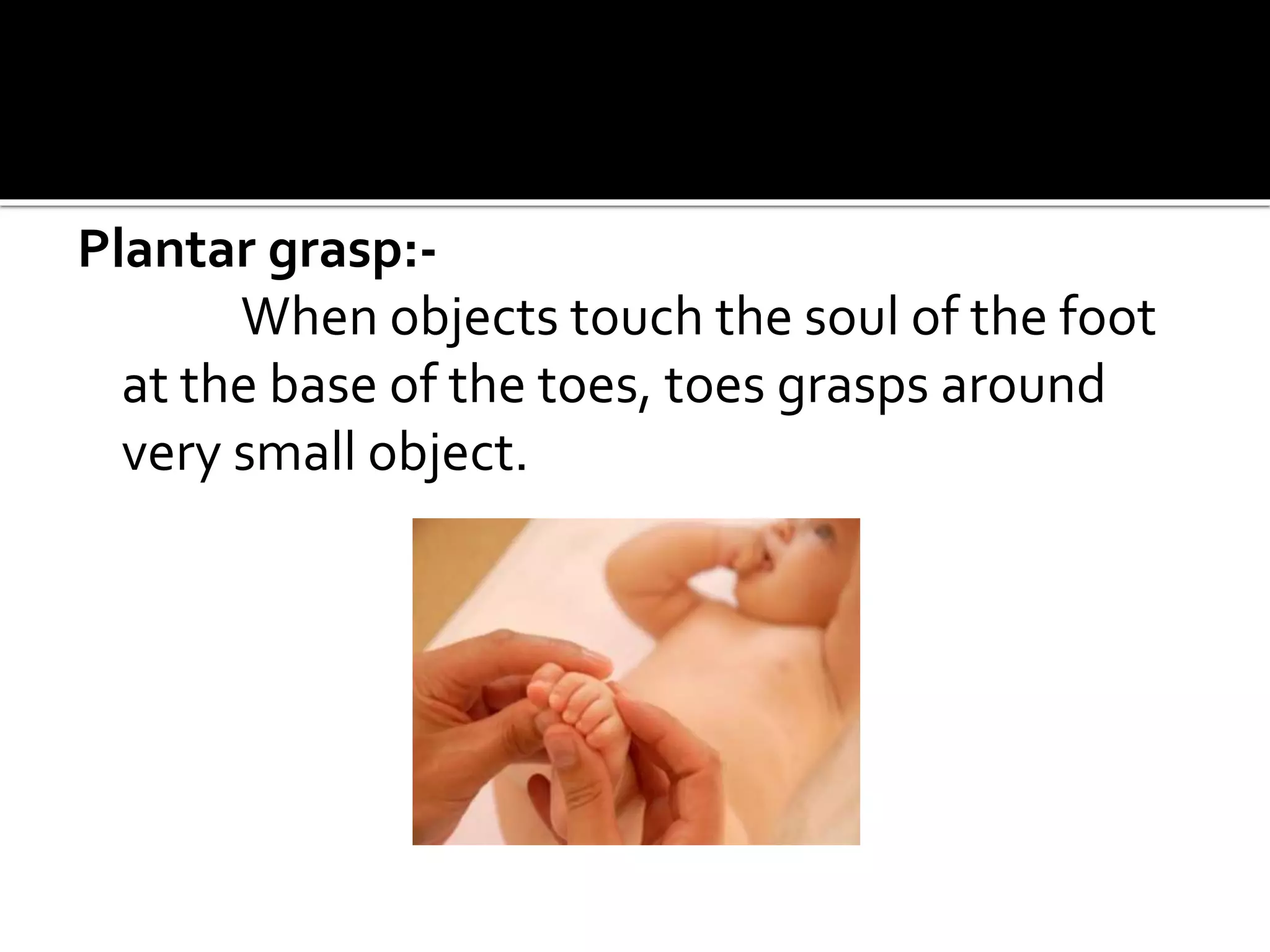
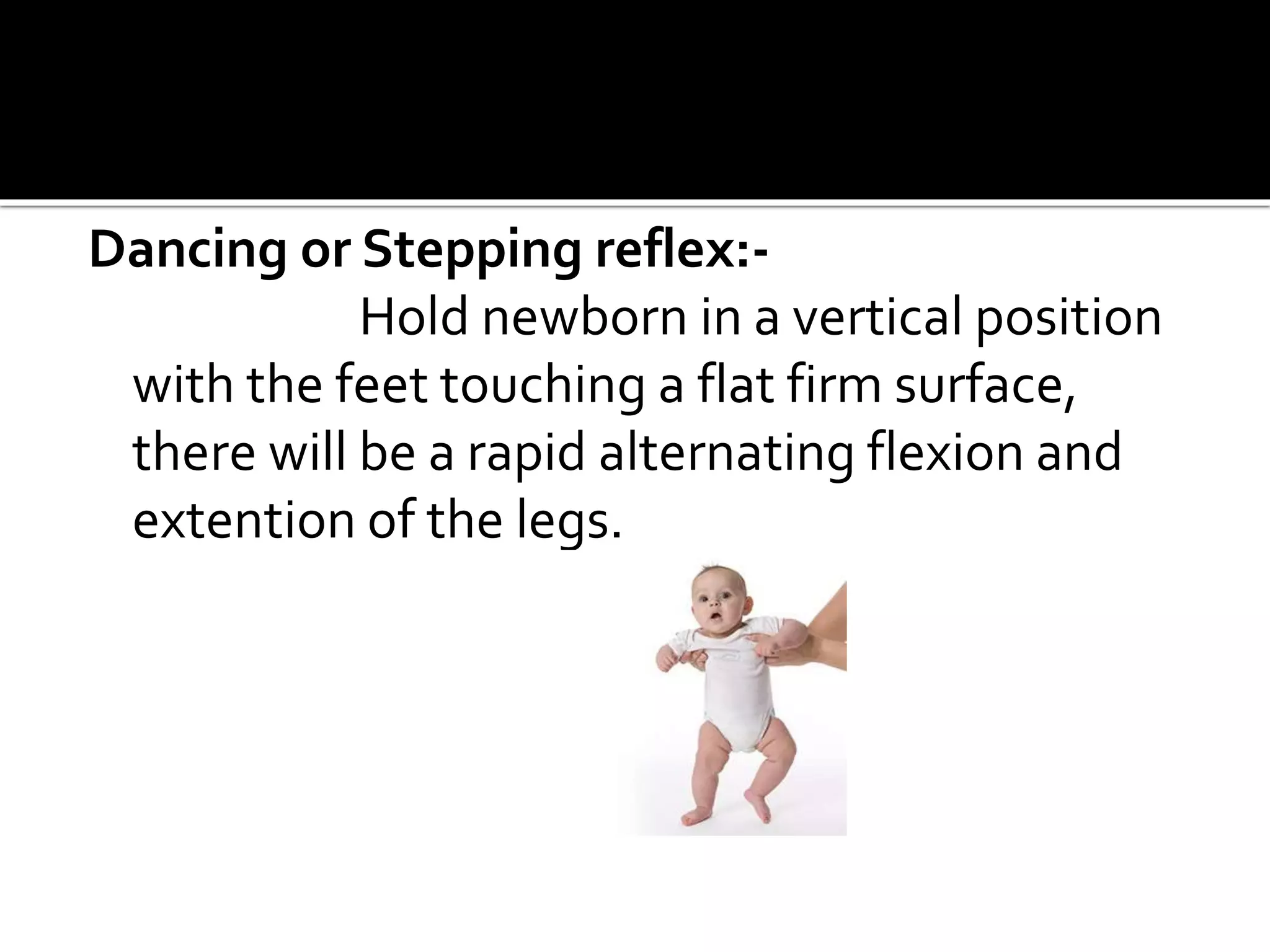
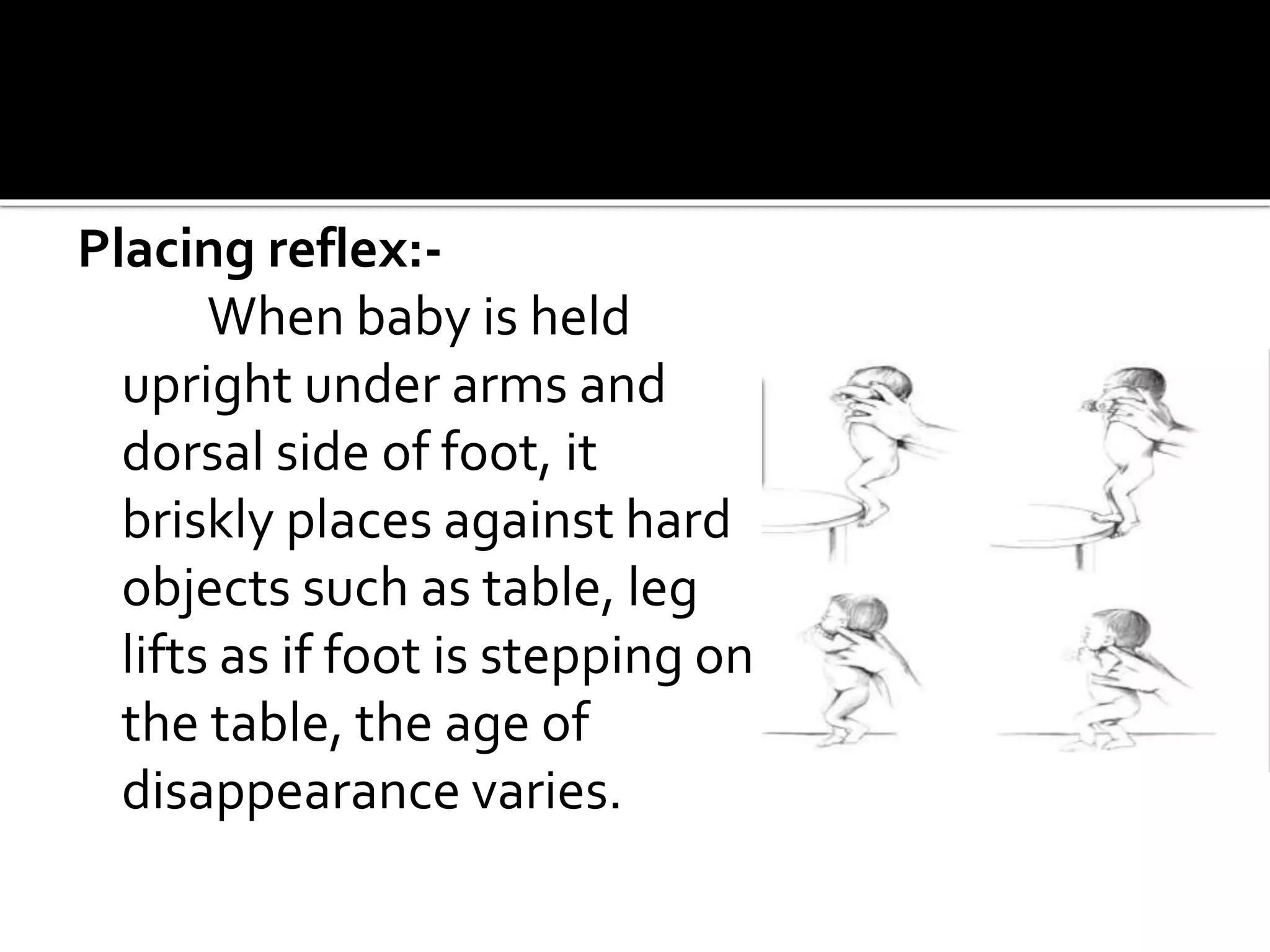
The document provides a comprehensive overview of human growth and development from birth through early childhood, outlining various reflexes, physical milestones, and developmental stages. It discusses psychosocial, psychosexual, spiritual, intellectual, and moral development across different ages, particularly emphasizing the changes in motor skills, language acquisition, and play behavior. Additionally, it highlights the importance of nurturing and securing environments that support growth and learning at each developmental stage.

































![Growth and Development with congenital anomalies [Lesson Plan] - Juhin J](https://cdn.slidesharecdn.com/ss_thumbnails/2fullcolumncontent-171014040923-thumbnail.jpg?width=640&height=640&fit=bounds)

















































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)


