The document discusses tuberculosis (TB) in pediatric patients, explaining its definition, stages, risk factors, pathophysiology, clinical presentation, diagnosis, and management options. It highlights that TB can be latent or active, with various symptoms and diagnostic methods tailored to children. Treatment regimens are detailed depending on HIV prevalence and isoniazid resistance, emphasizing appropriate dosages for children.
![PATHOPHYSIOLOGY
Inhalation of air borne mucus droplet nuclei 1-5 micron
in diameter.
10 -200 droplets can cause TB infection.
Droplet nuclei can stay in air for up to 72 hours in dark, damp room
[sunlight kills them].
When a person inhales droplet nuclei containing TB bacilli, they reach
the alveoli of the lungs.](https://image.slidesharecdn.com/gr12tuberculosisinpediatrics-240420021445-753e3b8b/85/GR-12-tuberculosis-in-pediatrics-pptx222-8-320.jpg)
![PATHOPHYSIOLOGY
These bacilli are ingested by alveoli macrophages, the majority of these bacilli
are destroyed or inhibited. A small number may multiply and are released when
the macrophages die.
These bacilli may spread to other parts of the lungs and through the lymphatic
channels or through the bloodstream to distant tissues and organs example;
pleural cavity, lymph nodes, kidneys, brain and bones.
The bacilli which goes in to the lungs causes pulmonary TB and the bacilli that
spreads to other parts of the body causes extra pulmonary TB [visceral TB,
bone and joint TB, cutaneous TB, CNS TB, perinatal TB].](https://image.slidesharecdn.com/gr12tuberculosisinpediatrics-240420021445-753e3b8b/85/GR-12-tuberculosis-in-pediatrics-pptx222-9-320.jpg)
![CLINICAL PRESENTATION
The presentation of TB in children differs from adults and also varies
within pediatric age groups [infants, toddlers, children, and adolescents]
as follows.
• Infants and children less than age 5 are more likely to develop TB once
infected than children five to ten years old.
Cough [2 weeks]
Fever[2weeks]
Night sweets](https://image.slidesharecdn.com/gr12tuberculosisinpediatrics-240420021445-753e3b8b/85/GR-12-tuberculosis-in-pediatrics-pptx222-10-320.jpg)
![MANAGEMENT
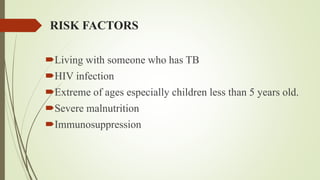
recommended treatment regimens for new cases of TB
TB Diagnostic Category Anti-TB drug regimen
Intensive phase Continuation
phase
Low HIV prevalence [and HIV- negative children and low isoniazid resistance settings
Smear-negative pulmonary TB
Intrathoracic lymph node TB
Tuberculosis peripheral lymphadinitis
2HRZ 4HR
Extensive pulmonary disease
Smear-positive pulmonary TB
Severe forms of extrapulmonary TB [other than tuberculosis
meningitisosteoarticular TB].
2HRZE 4HR
High HIV prevalence or high isoniazid resistance or both
Smear-positive PTB
Smear-negative PTB with ir without extensive parenchymal disease
All forms of EPTB except tuberculosis meningitis and osteoarticulat TB
2HRZE 4HR
Tuberculosis meningitis and osteoarticular TB in all regions 2HRZE 10HR](https://image.slidesharecdn.com/gr12tuberculosisinpediatrics-240420021445-753e3b8b/85/GR-12-tuberculosis-in-pediatrics-pptx222-13-320.jpg)
![TREATMENT CONT….
Doses of Anti-TB Drugs
As children approach a body weight of 25kg, adult dosages can be used
Drugs Suggested daily dose
Isoniazid 10[7-15] mgkg
Rifampicin 15[10-20] mgkg
Pyrazinamide 35[30-40] mgkg
Ethambutol 20[15-25] mgkg](https://image.slidesharecdn.com/gr12tuberculosisinpediatrics-240420021445-753e3b8b/85/GR-12-tuberculosis-in-pediatrics-pptx222-14-320.jpg)
























































![ACUTE_AND_CHRONIC_RENAL_FAILxxxxx1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/acuteandchronicrenalfail1-250803044151-1ee4884c-thumbnail.jpg?width=640&height=640&fit=bounds)































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)