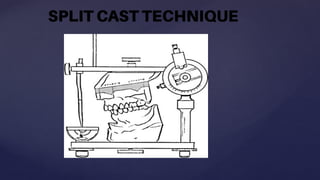
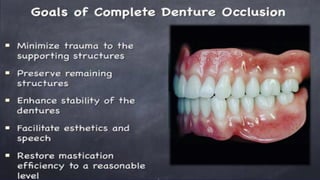
The document outlines the clinical steps for achieving balanced occlusion in complete dentures, emphasizing the importance of minimizing movement to reduce trauma to supporting tissues and improve patient comfort. Key procedures include establishing vertical and horizontal jaw relations, using face bow transfers, and employing techniques such as gothic arch tracing and split cast techniques to verify centric relation. The document also discusses the significance of incisal guidance and the impact of condylar guidance on jaw separation during protrusion, highlighting the need for careful adjustment in denture construction.

















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








