Downloaded 64 times




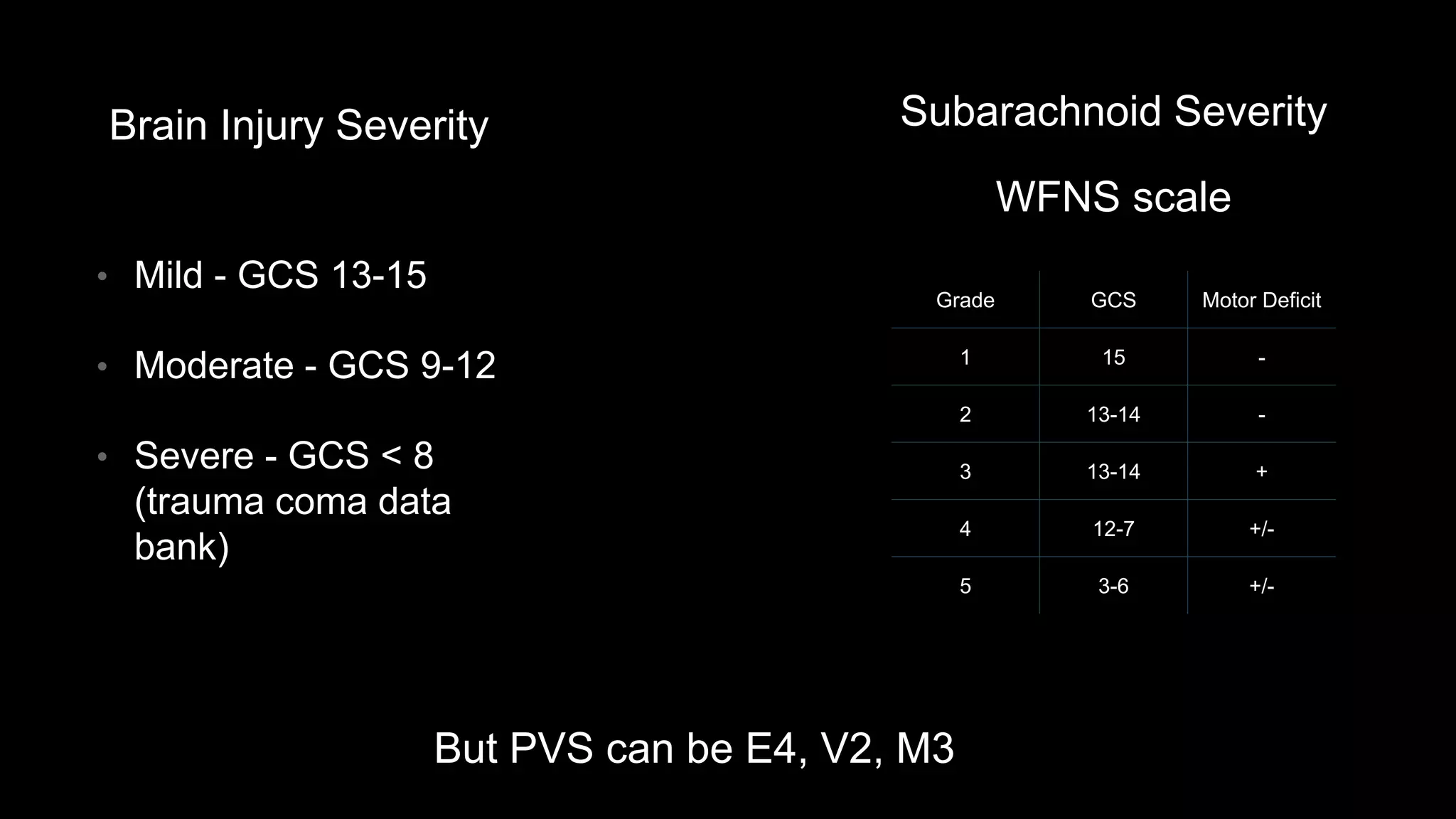























The document discusses the Glasgow Coma Scale (GCS) and its application in assessing levels of consciousness from wakefulness to coma. It highlights the significance of GCS in communication, prognosis, and measuring head injury severity, while also addressing its limitations and the need for considering underlying pathologies. Future directions include exploring advanced imaging and assessment techniques beyond traditional scoring methods.
































































































