

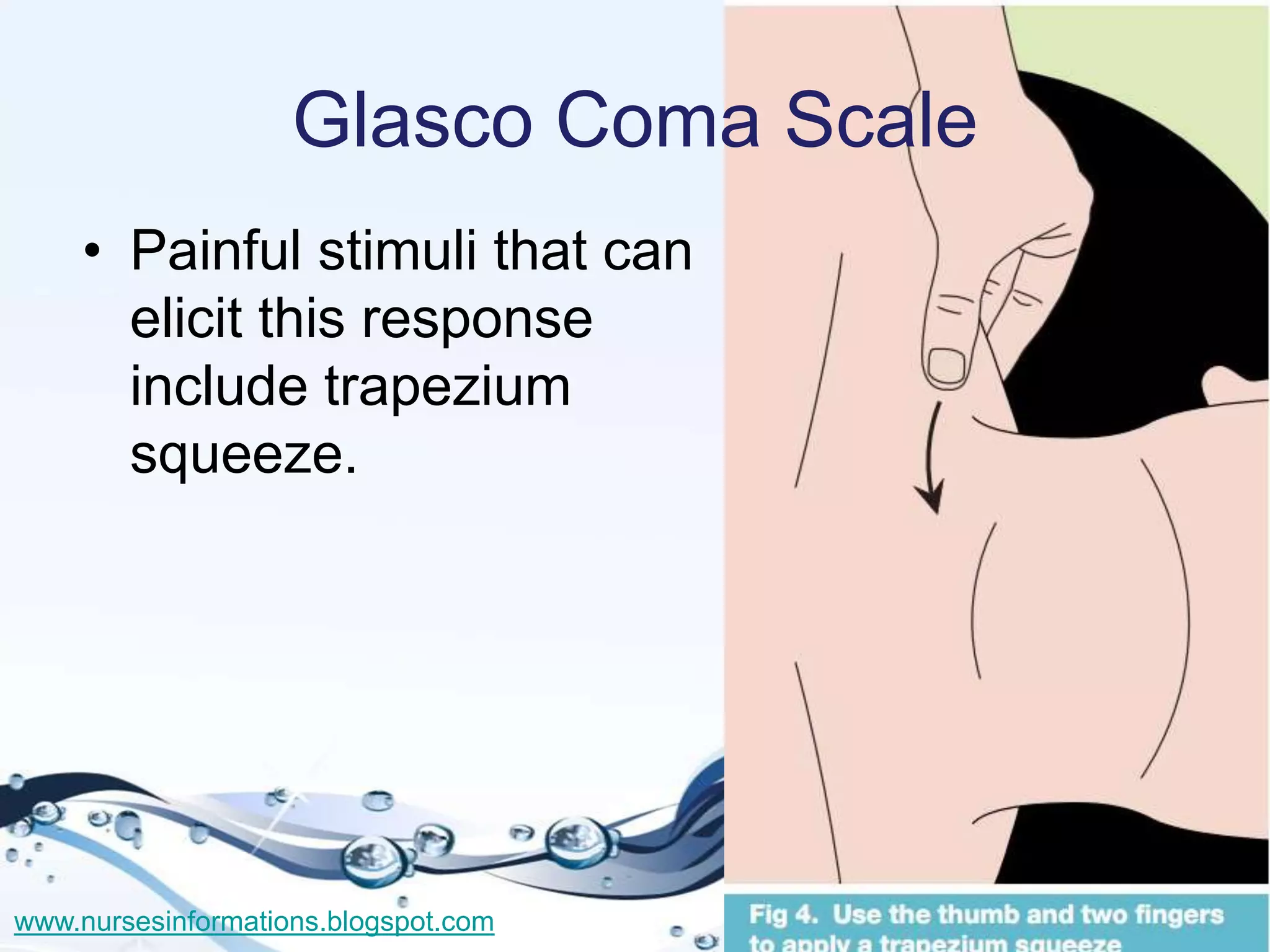
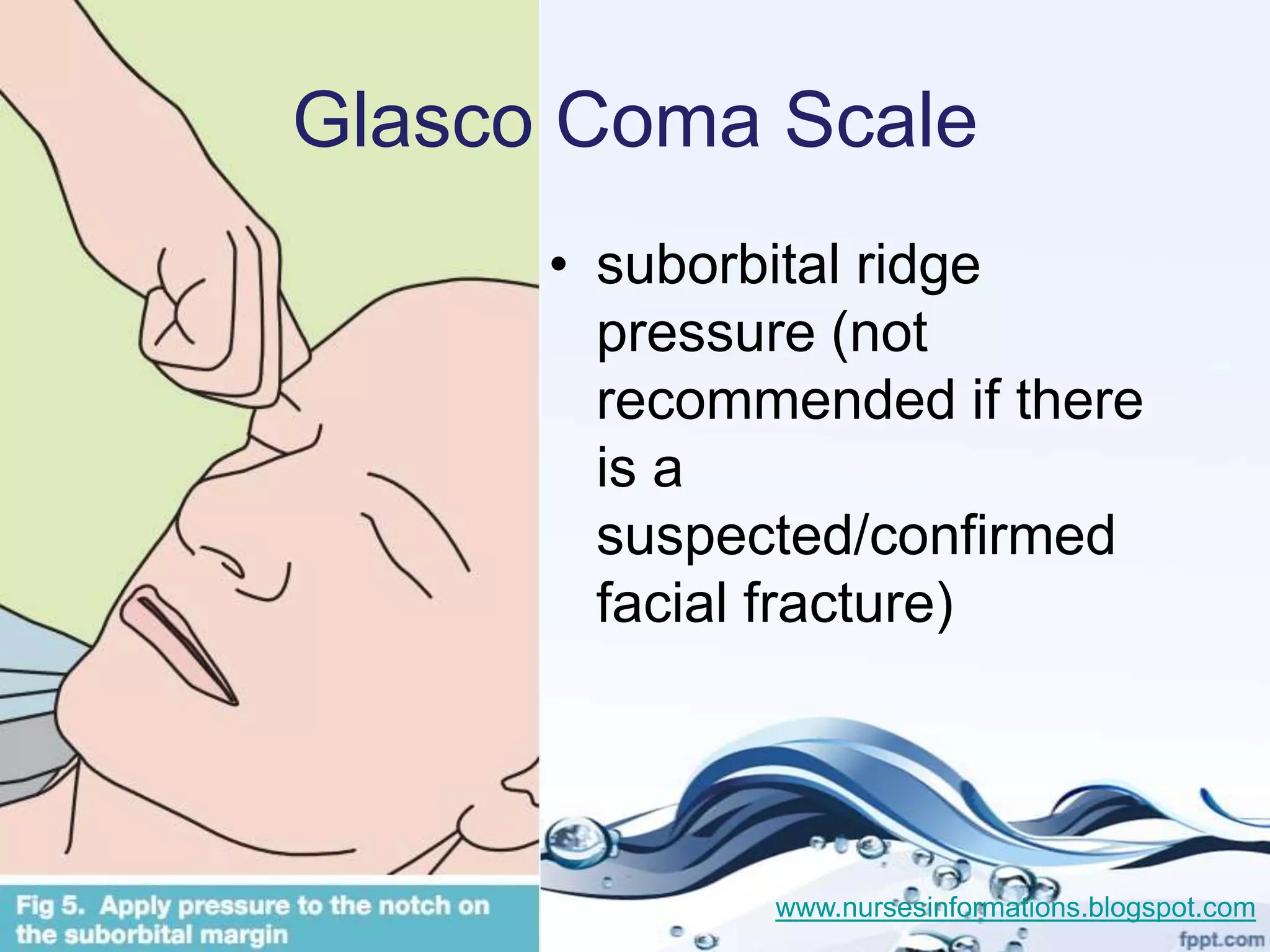
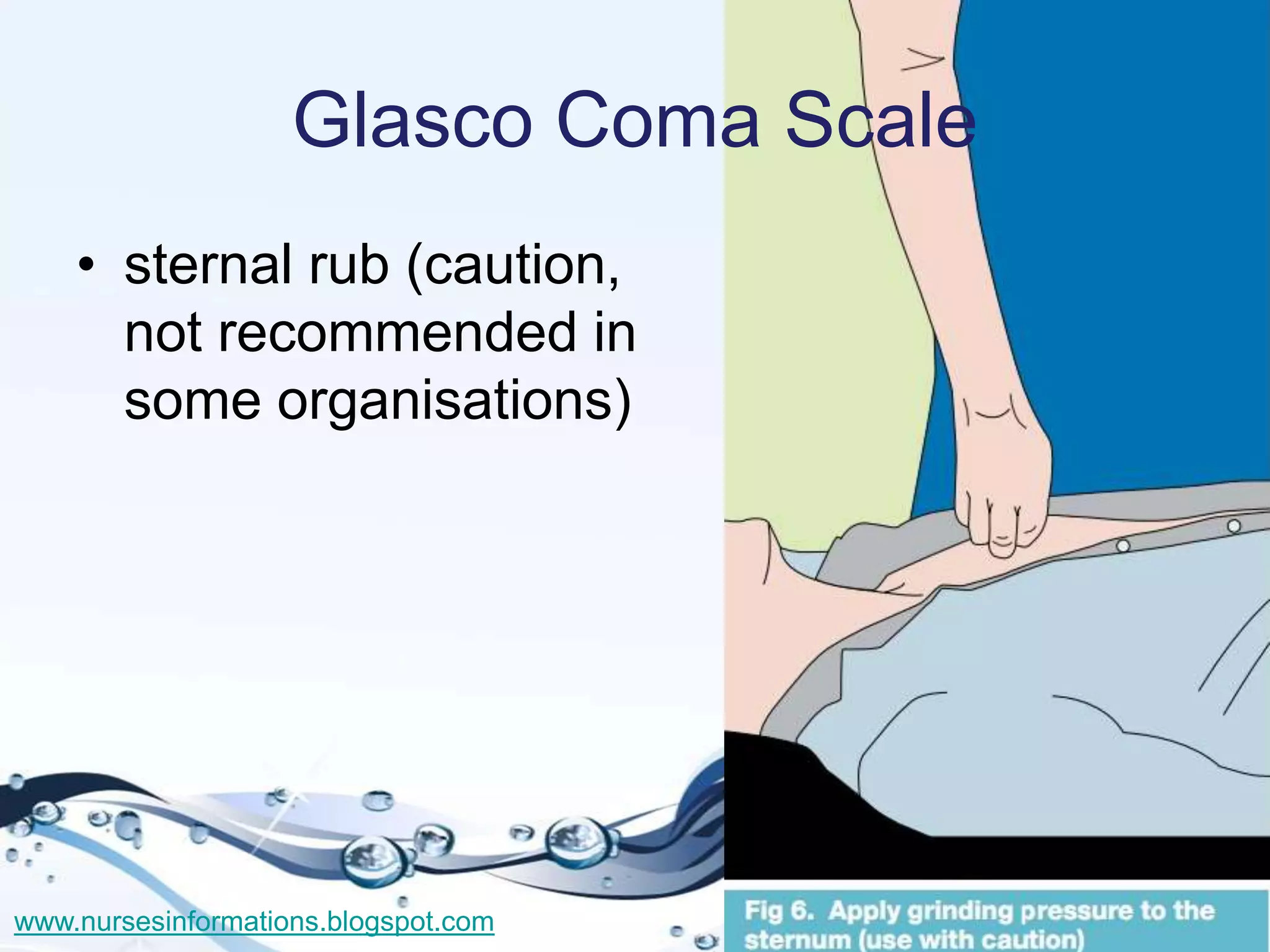
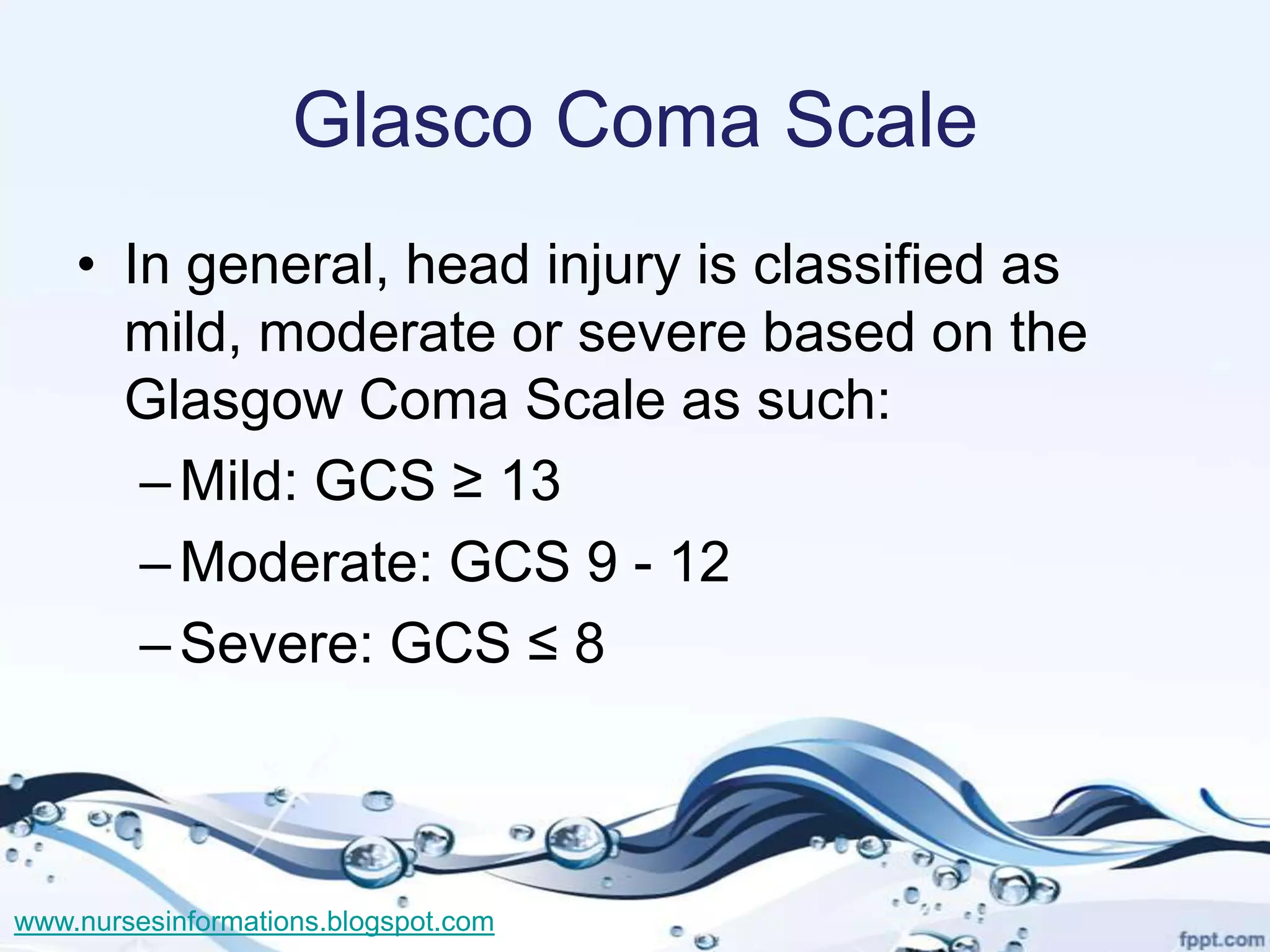
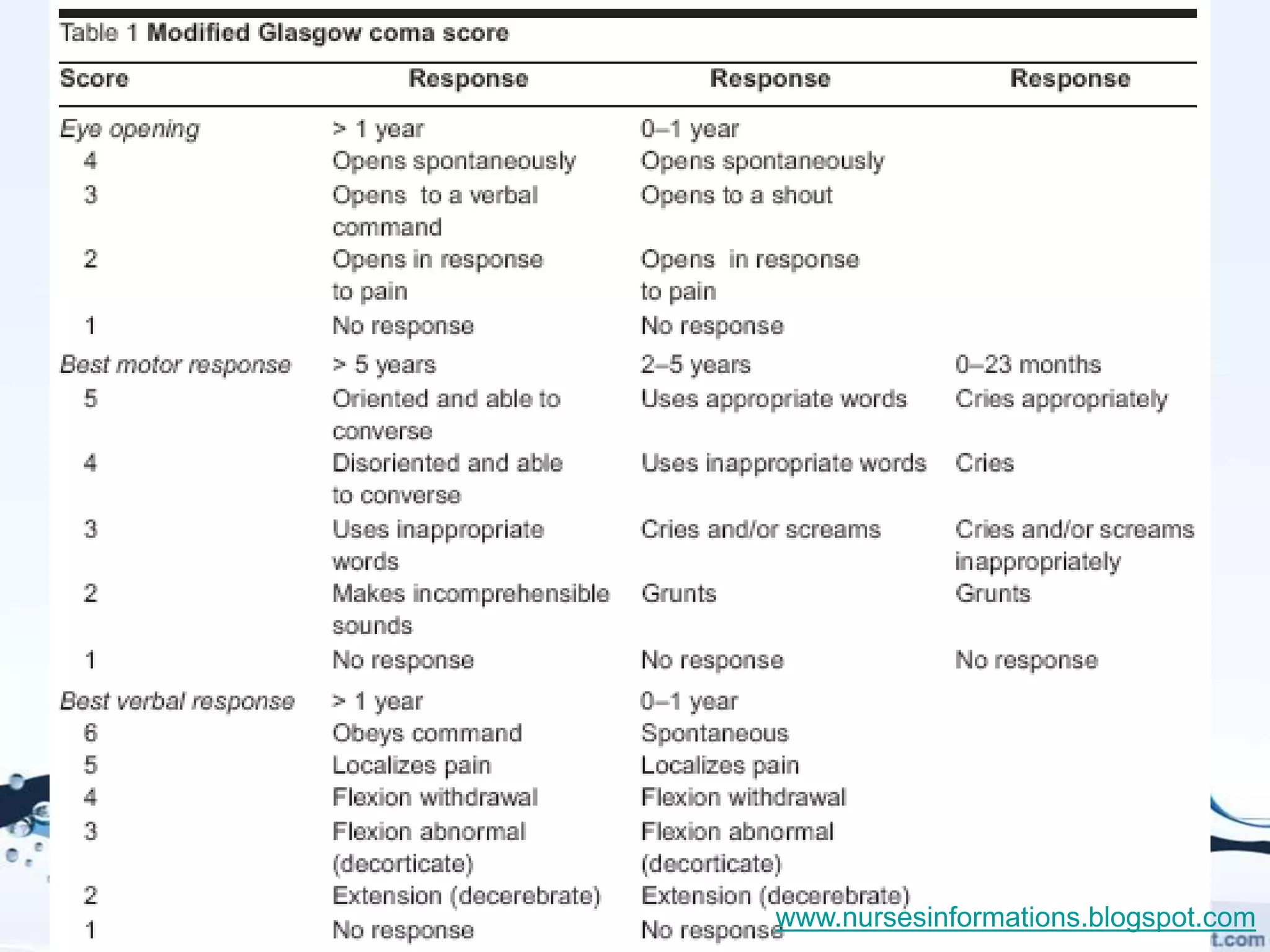



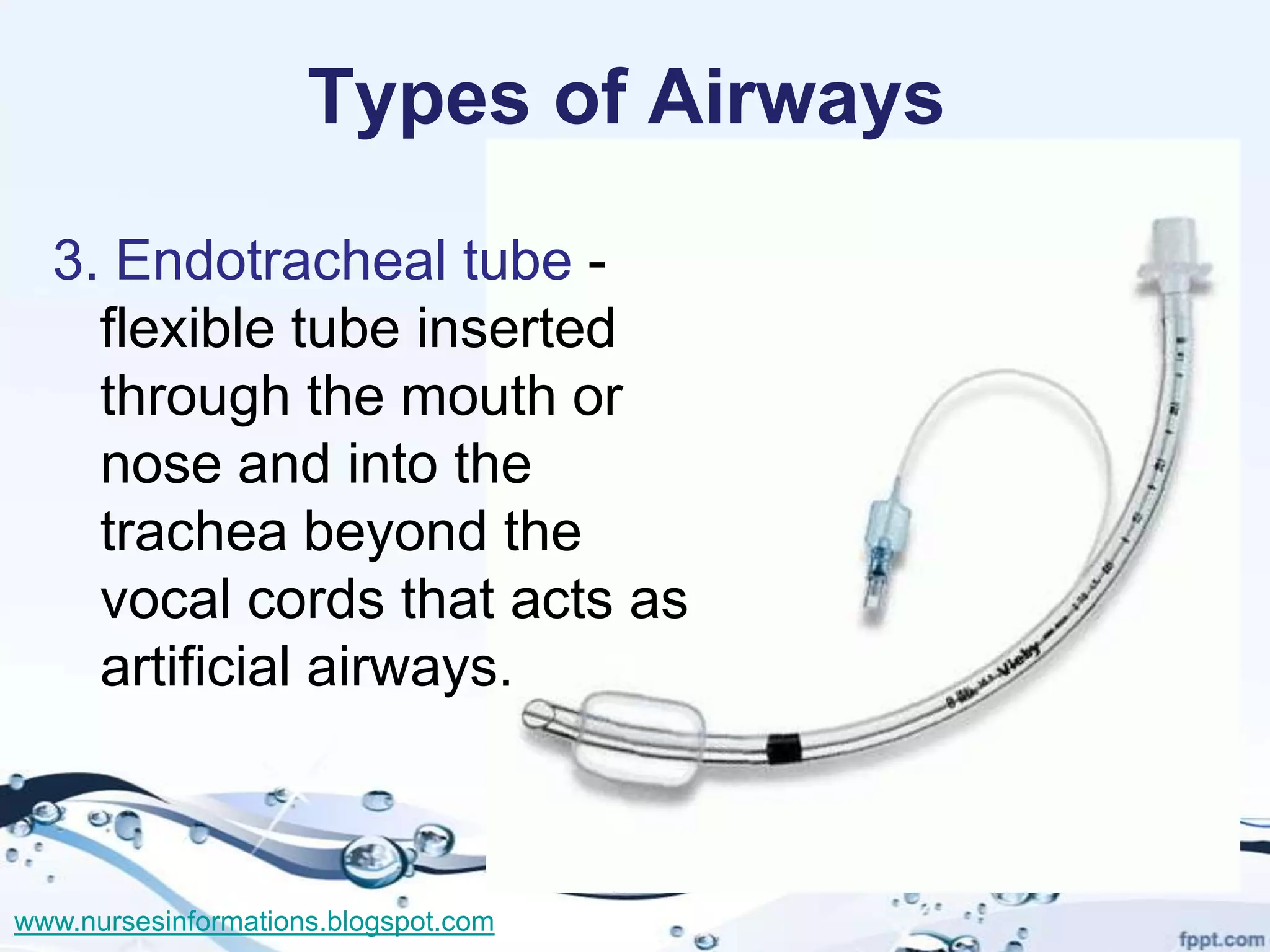
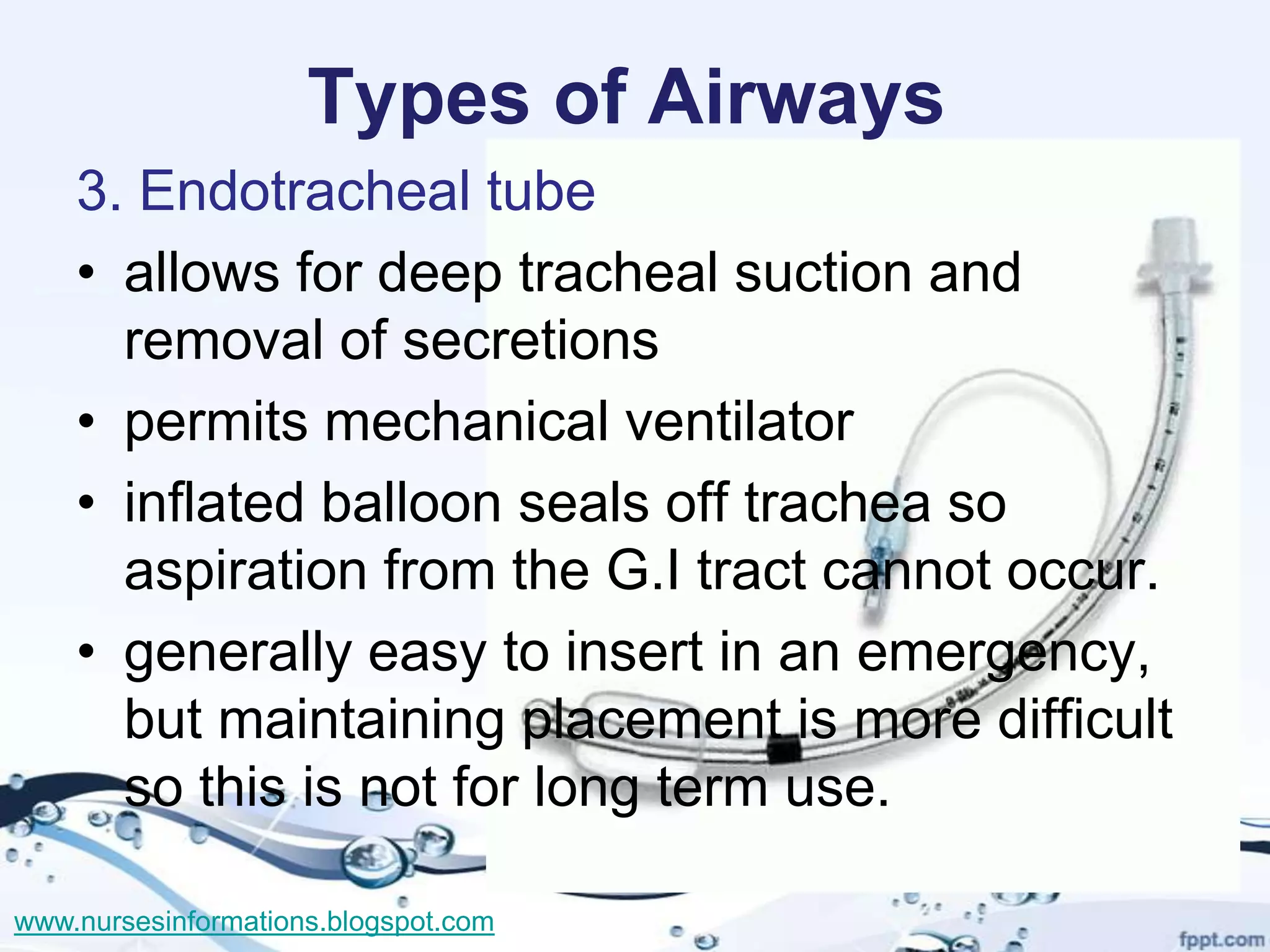

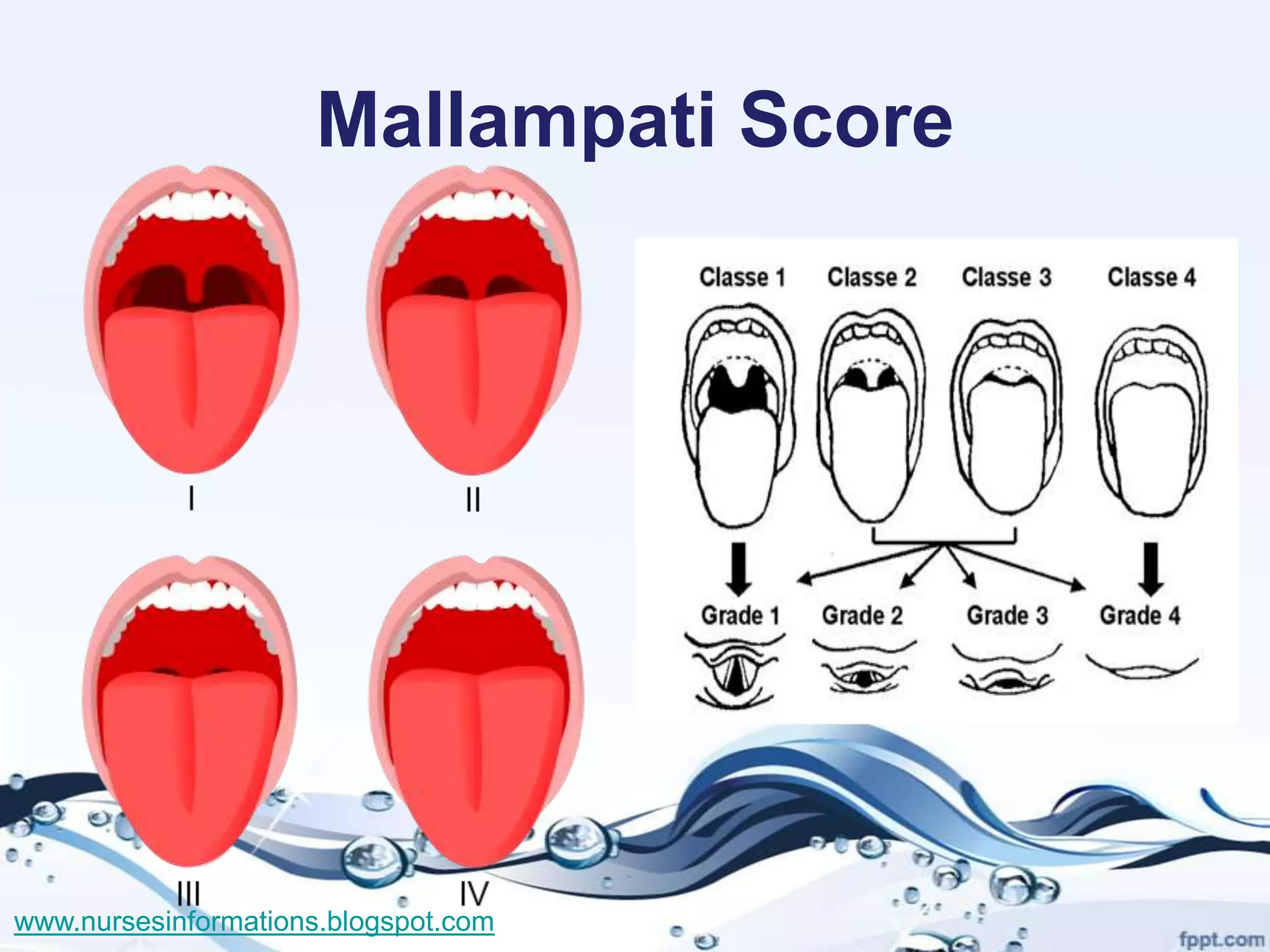
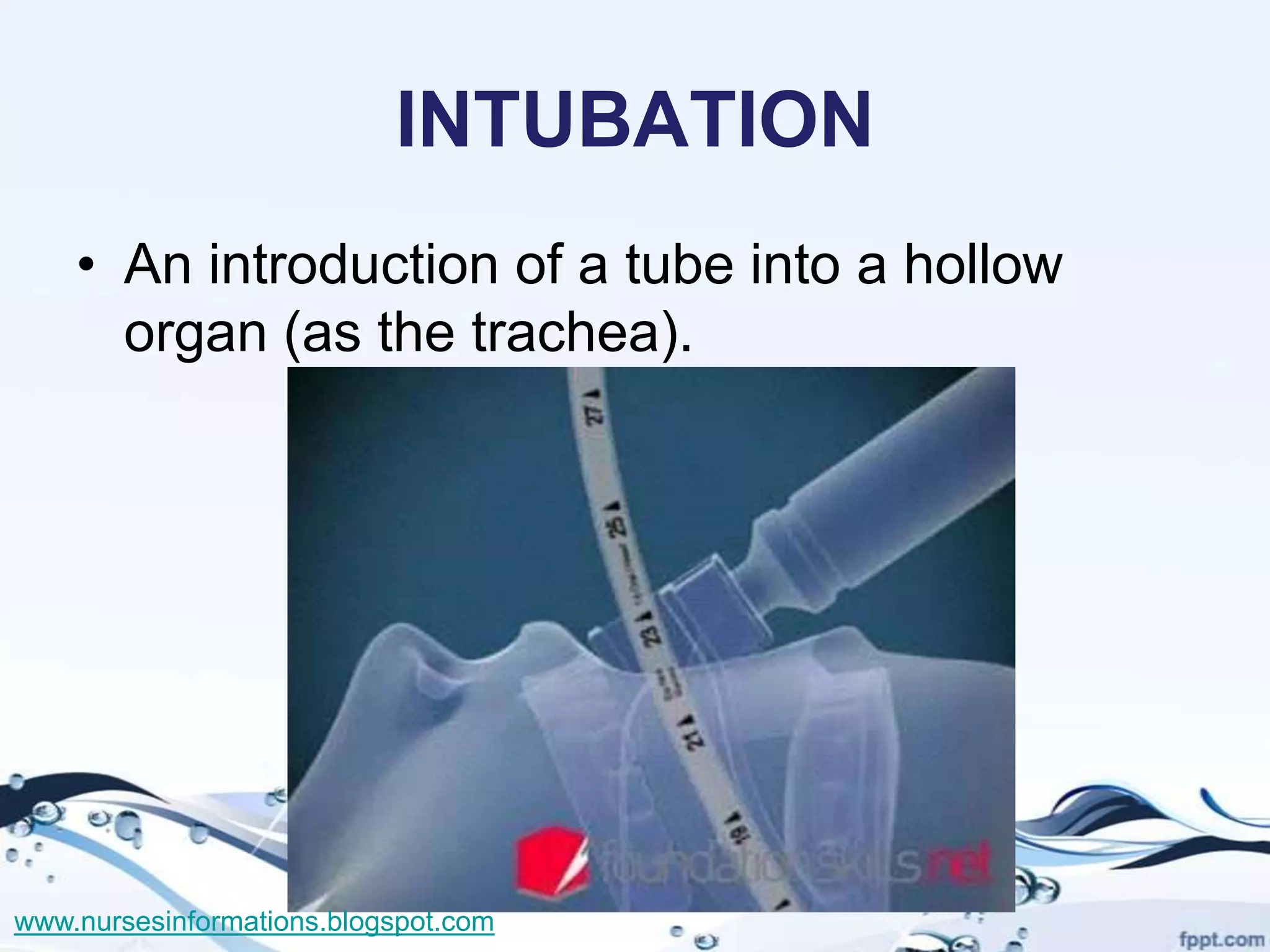
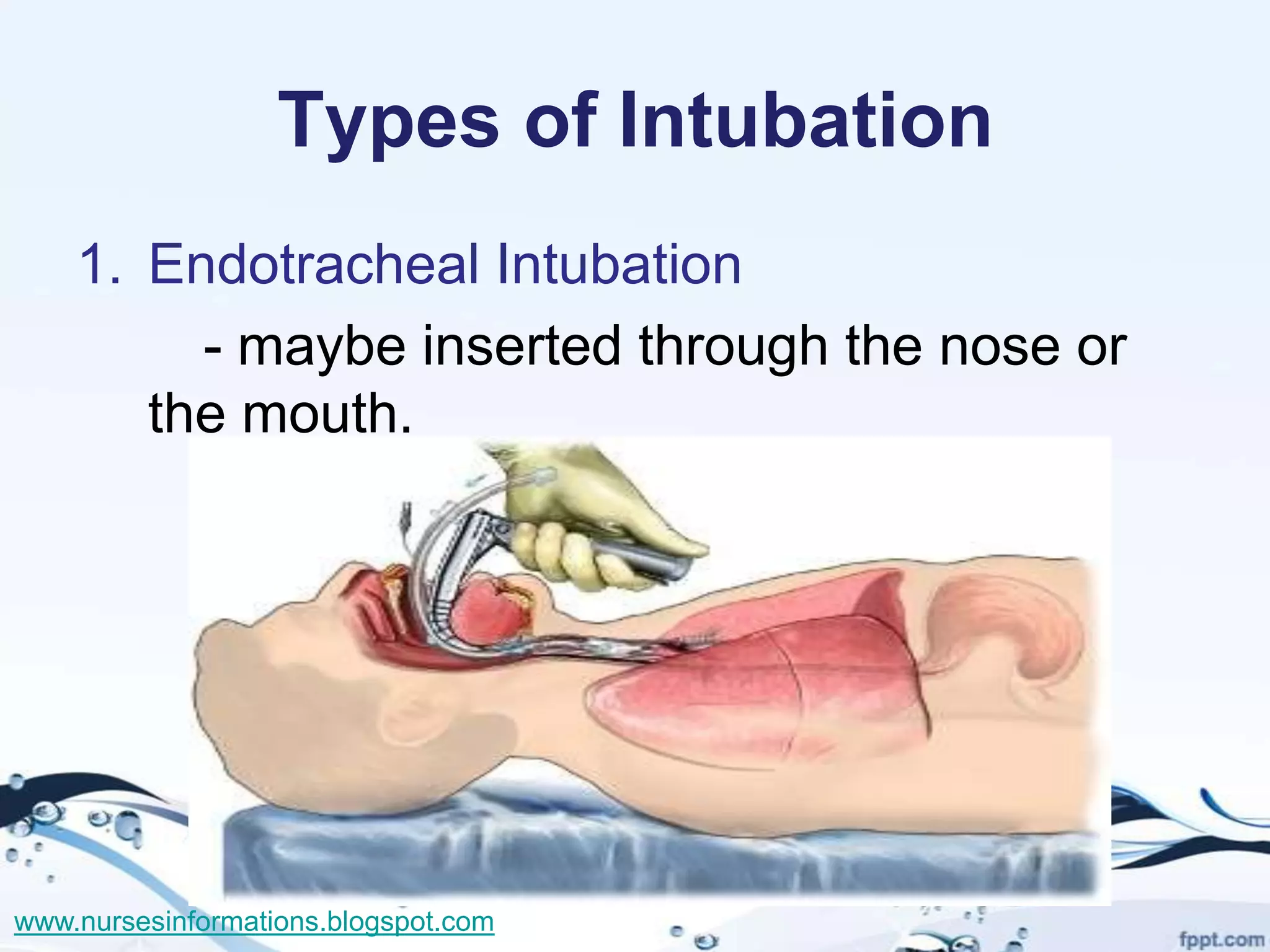
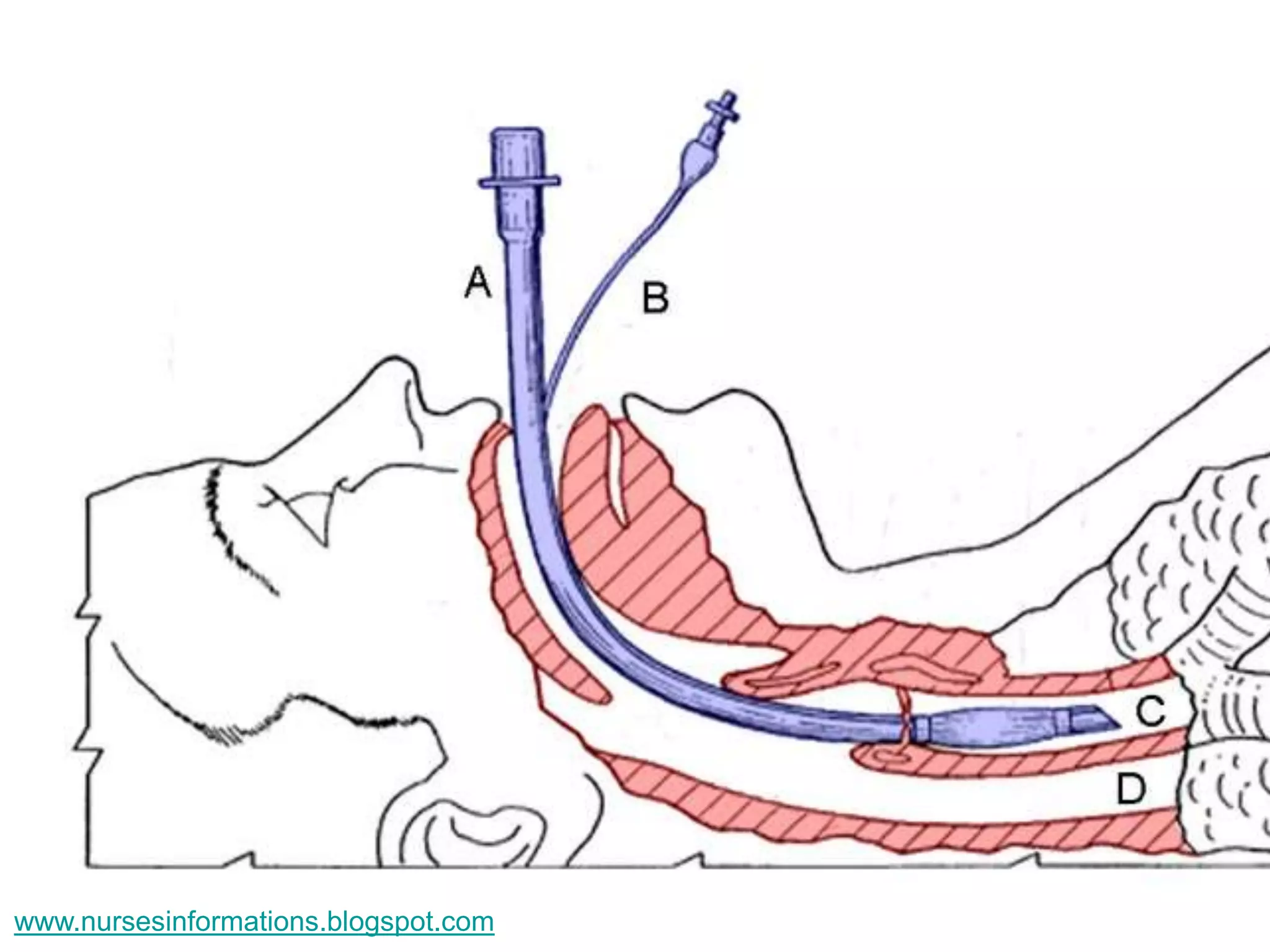

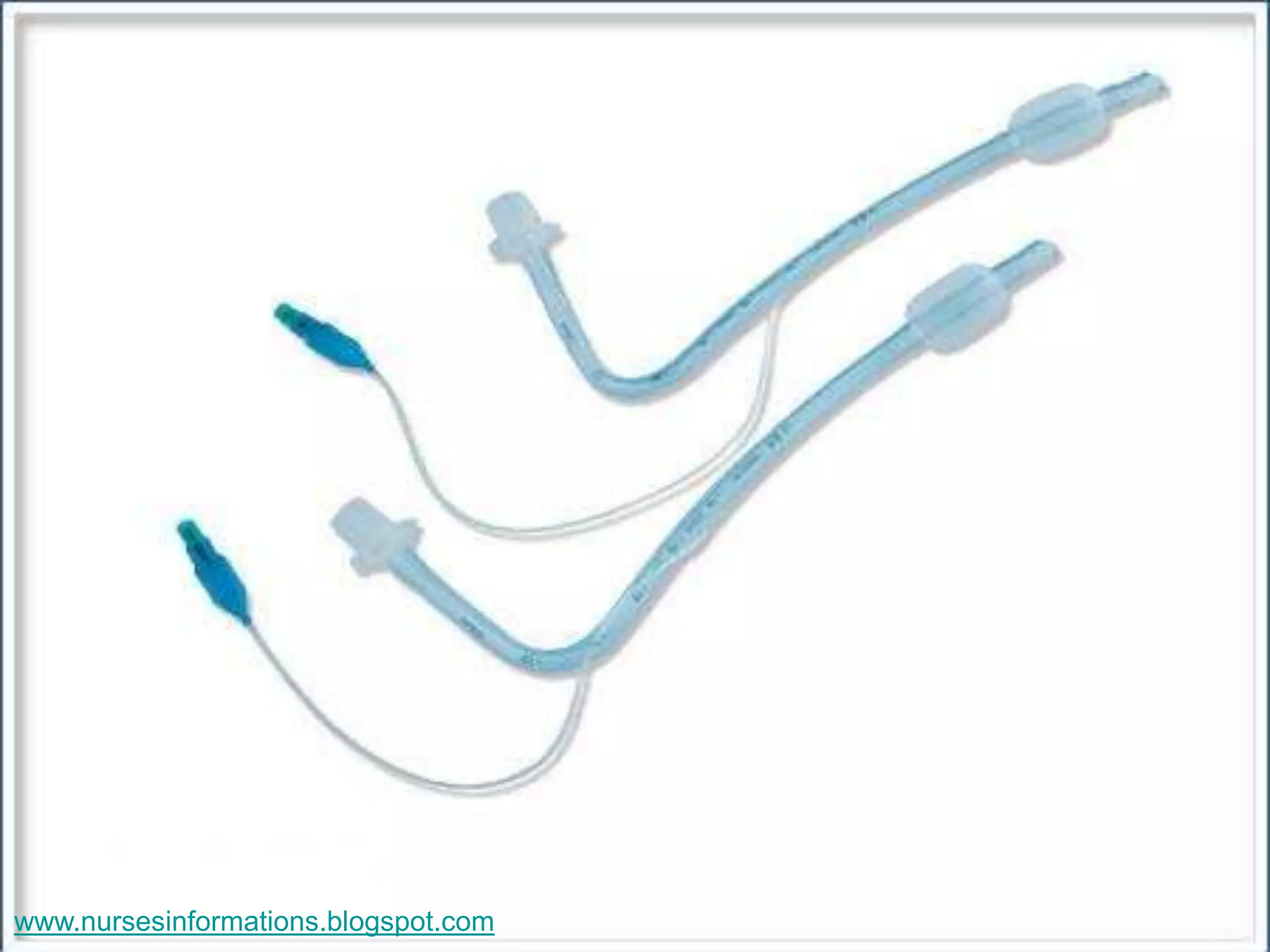
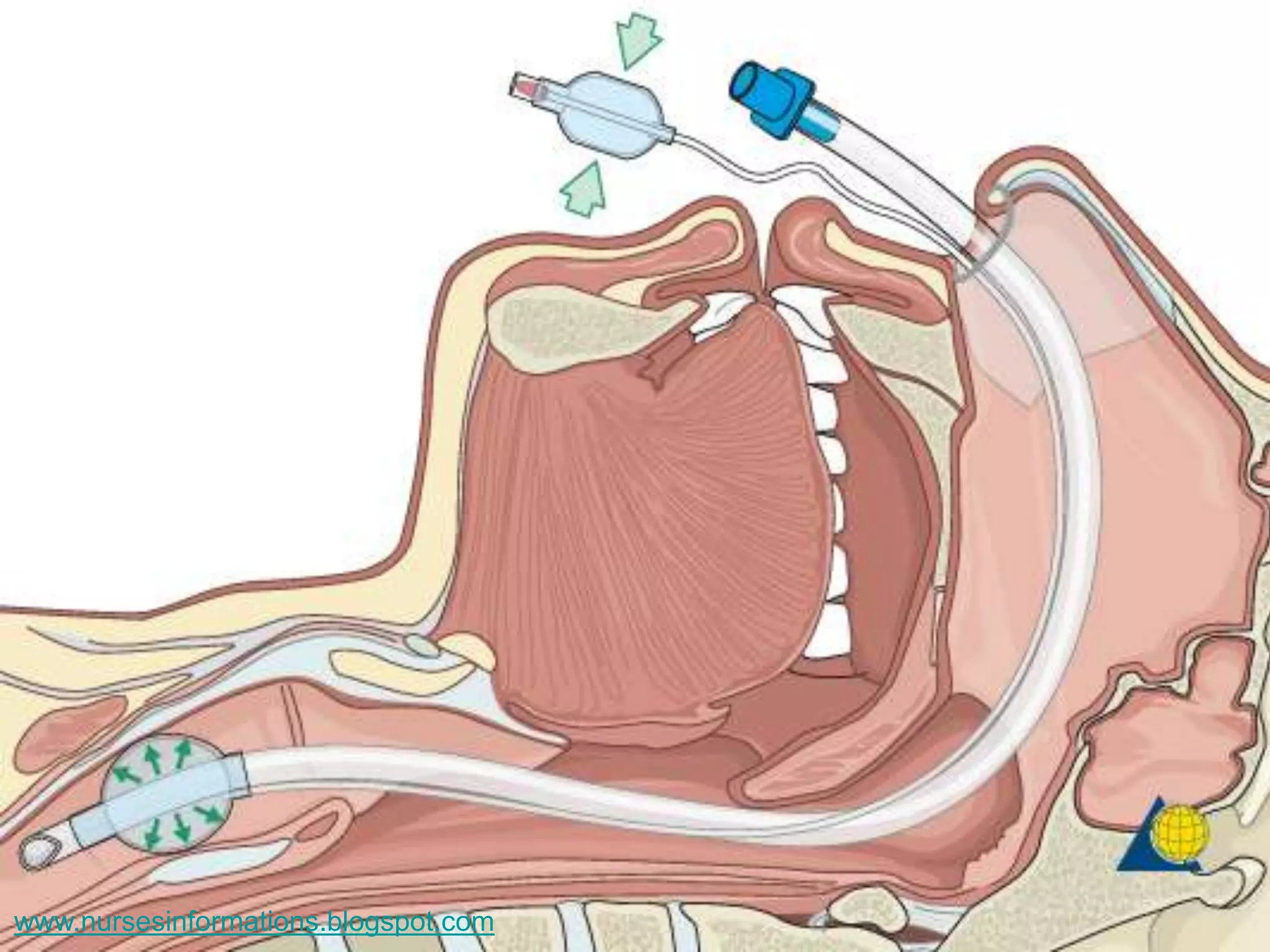


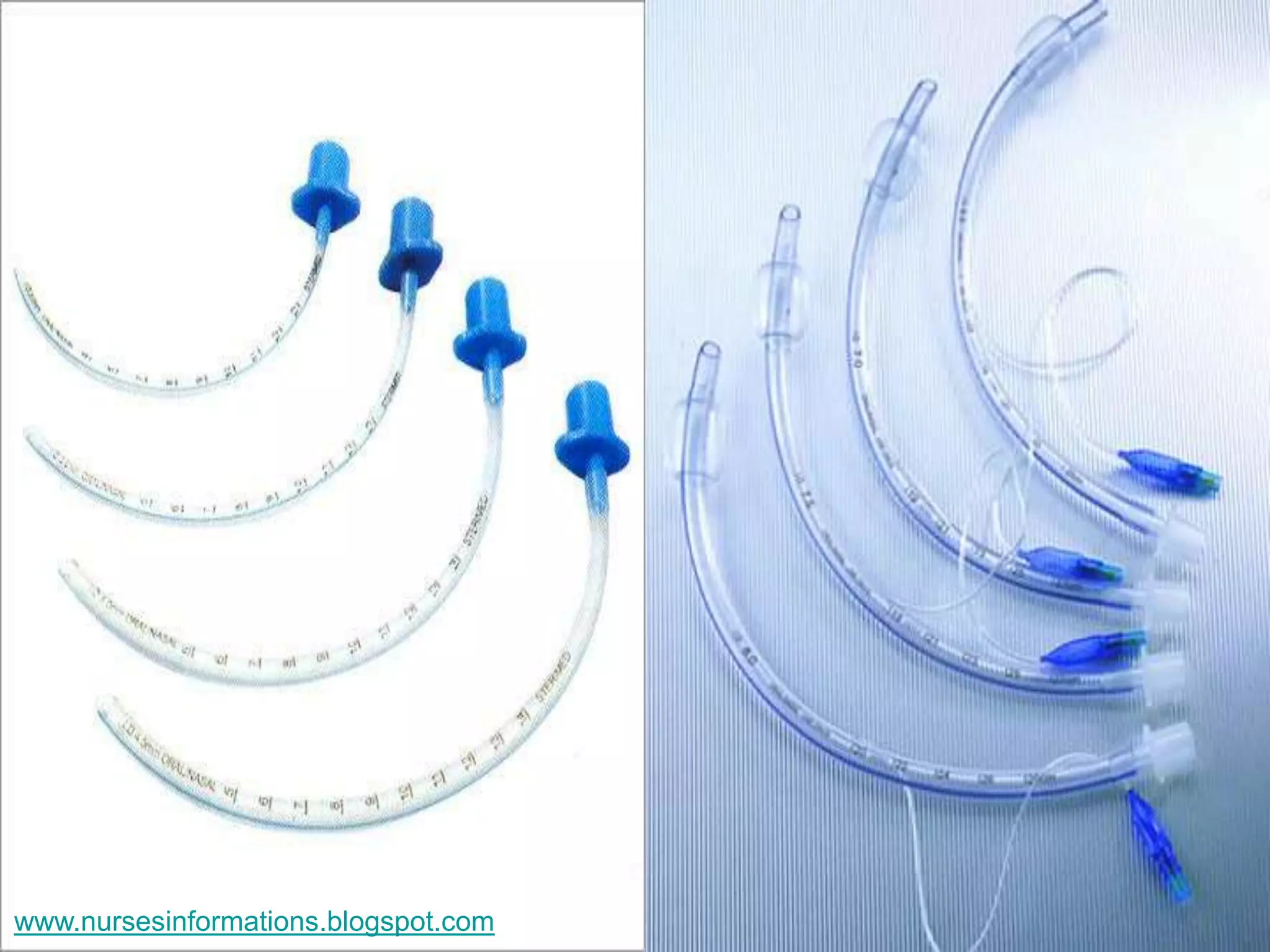


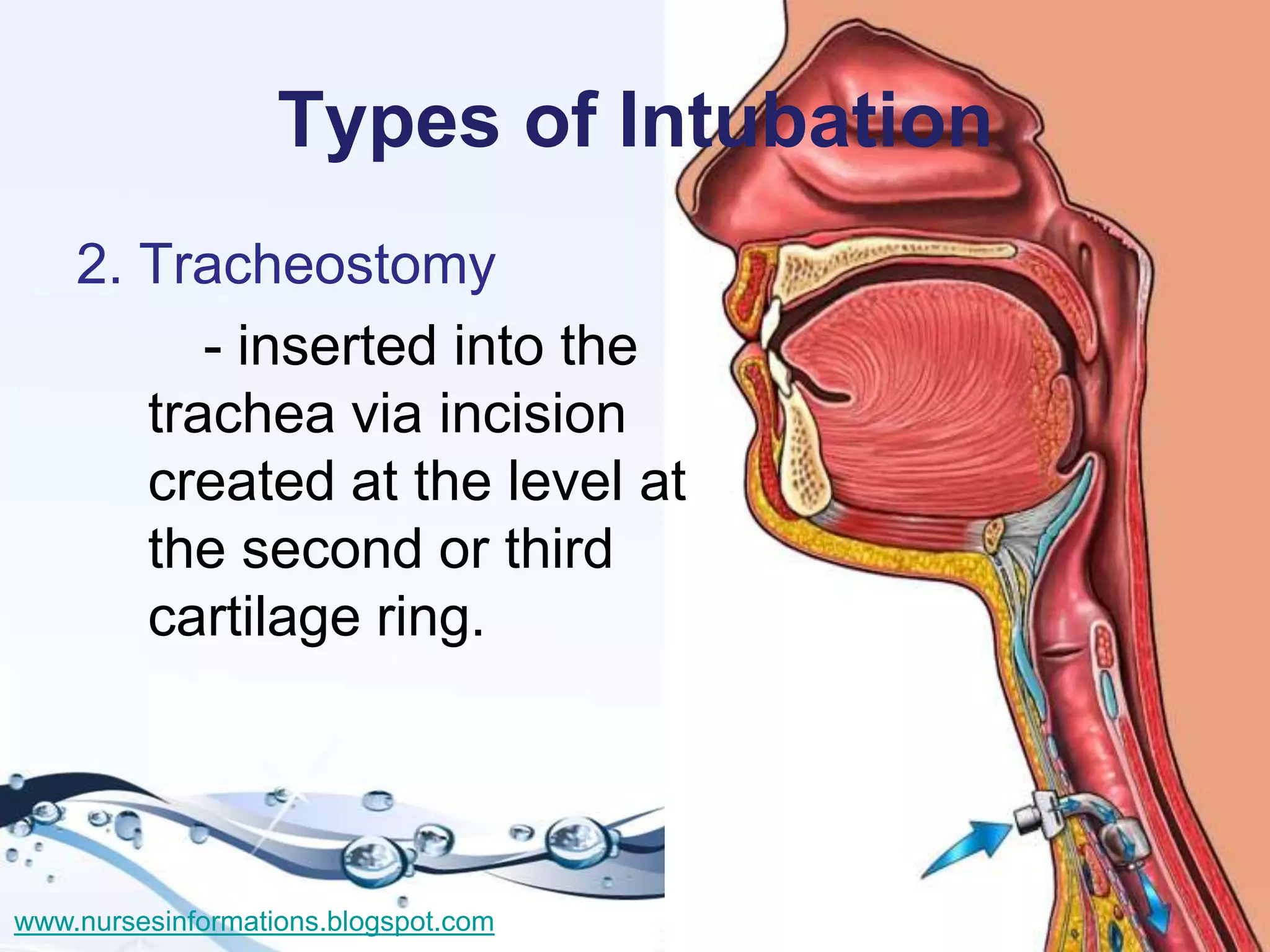


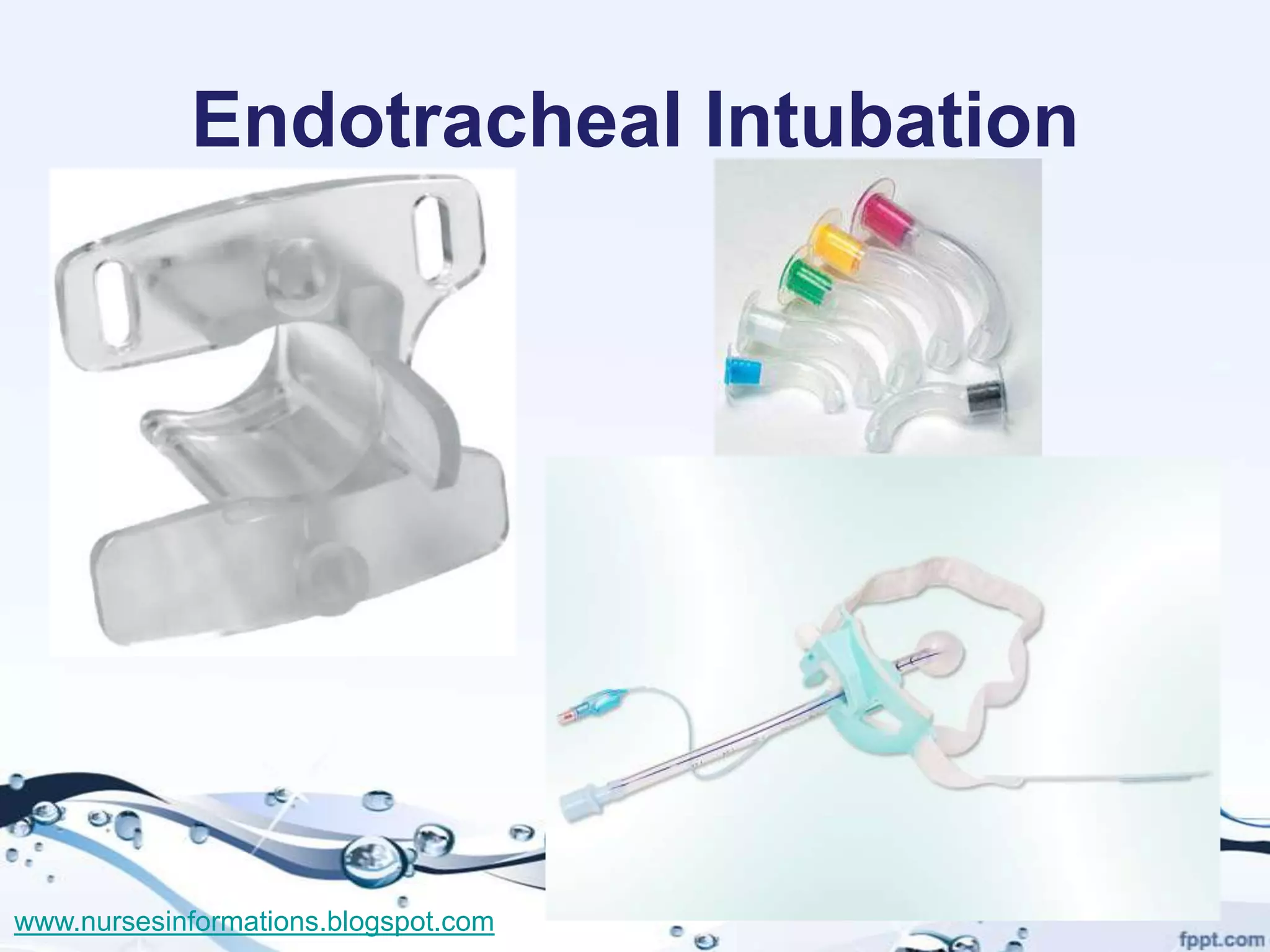





The document provides a comprehensive overview of the Glasgow Coma Scale (GCS) for assessing consciousness in patients, particularly those with head injuries, using a scoring system from 3 to 15 based on eye opening, verbal response, and motor response. It also discusses various types of airways, indications for intubation, and the Mallampati score used to predict intubation difficulty. Additionally, it details the procedures for endotracheal intubation and tracheostomy, including necessary equipment and steps involved.





































































































