Definition
• The GlasgowComa Scale
(GCS) is a neurological
scoring system used to
objectively measure a
patient’s level of
consciousness (LOC) after a
head injury or any condition
affecting the brain.
4.
Definition
• It assesseshow awake, responsive, and aware a
person is by observing three key functions:
• Eye opening (E)
• Verbal response (V)
• Motor response (M)
5.
Purpose
To quantify consciousnessin a
standardized, reproducible way.
To help communicate the patient’s
neurological status clearly among
healthcare professionals.
To monitor changes over time which may be
improvement or deterioration.
To guide management decisions in
traumatic brain injury (TBI).
6.
History and
Developme
nt
Before 1970,assessing a patient’s level of
consciousness was highly subjective.
Doctors would describe patients with
vague terms like:“He’s drowsy," “She’s
semiconscious," "He’s obtunded.”
These terms were ambiguous, non-
standardized, and difficult to compare
between hospitals or studies.
This inconsistency made it hard to track
neurological progress or predict
outcomes in head injury patients.
7.
History and
Developme
nt
The GlasgowComa Scale was
introduced in 1974 by
Professor Graham Teasdale (a
neurosurgeon) and Professor
Bryan Jennett (a neurologist).
Both were from the Institute of
Neurological Sciences,
University of Glasgow,
Scotland.
8.
Component
s of GCS
•The Glasgow Coma Scale
(GCS) assesses a patient’s
level of consciousness
through three key
responses:
A. Eye Opening Response
(E) – 4 points
• What It Tests: Brainstem
function and arousal
mechanism of the reticular
activating system.
SCORE RESPONSE CLINICAL
MEANING
4 Opens eyes
spontaneously
Fully awake and
alert
3 Opens eyes to
speech
Responds when
spoken to
2 Opens eyes to
pain
Responds only
to painful
stimulus
1 No eye opening Deep coma/
brain
dysfunction
9.
Eye
Opening
Response
How to Test:
Observeif eyes open spontaneously.
If not, call the patient’s name or give a
loud verbal command.
If no response, apply a painful stimulus
(e.g., trapezius pinch or supraorbital
pressure).
Record the best eye response.
10.
Components
of GCS
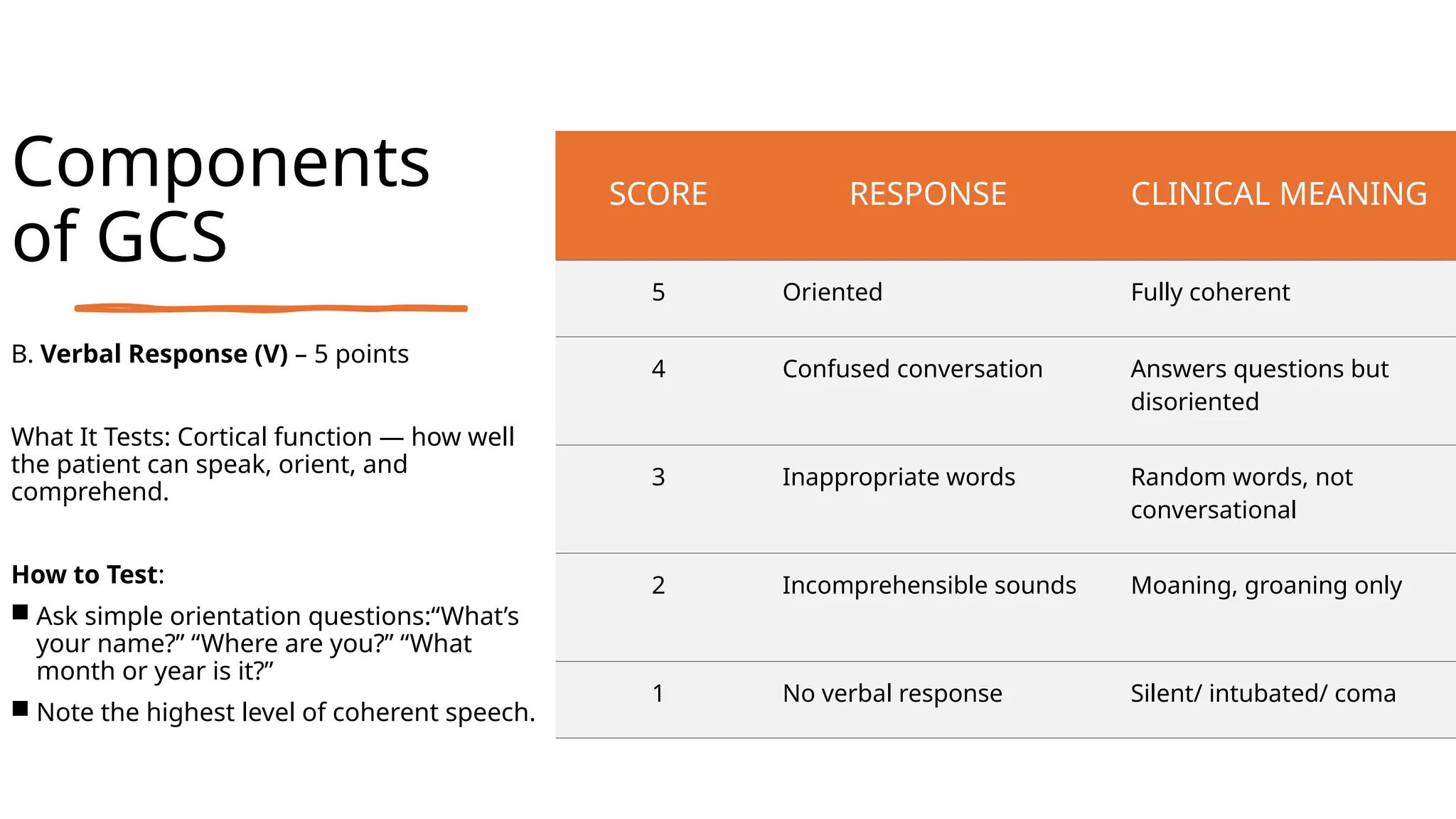
B. VerbalResponse (V) – 5 points
What It Tests: Cortical function — how well
the patient can speak, orient, and
comprehend.
How to Test:
Ask simple orientation questions:“What’s
your name?” “Where are you?” “What
month or year is it?”
Note the highest level of coherent speech.
SCORE RESPONSE CLINICAL MEANING
5 Oriented Fully coherent
4 Confused conversation Answers questions but
disoriented
3 Inappropriate words Random words, not
conversational
2 Incomprehensible sounds Moaning, groaning only
1 No verbal response Silent/ intubated/ coma
11.
Verbal
Response (V)
• Example:
•If patient says, “I’m at home”
(while in hospital), score V4.
• For Infants/Non-verbal
children:
• Use Modified Pediatric GCS
— e.g., coos and babbles
(V5), cries to pain (V2), etc.
12.
Motor
Response (M)
C. MotorResponse (M)
– 6 points
• What It Tests: Integrity
of corticospinal tracts
and ability to respond
purposefully.
SCORE RESPONSE CLINICAL
IMPLICATION
6 Obeys command Purposeful
movement
5 Localized pain Moves hand
towards site of
pain
4 Withdraws from
pain
Pulls limb away
3 Flexion
( decorticate
posture)
Abnormal Flexion
to pain
2 Extension
(reverberate
posture)
Abnormal
Extension to pain.
13.
Motor
Response (M)
How toTest:
• Give a simple command: “Lift your
hand,” “Squeeze my finger.”
• If no response, apply pain stimulus:
. Central: trapezius pinch or
supraorbital pressure.
Peripheral: nail bed pressure.
• Observe if patient localizes,
withdraws, or shows abnormal
posturing.
14.
Scoring and
Interpretation
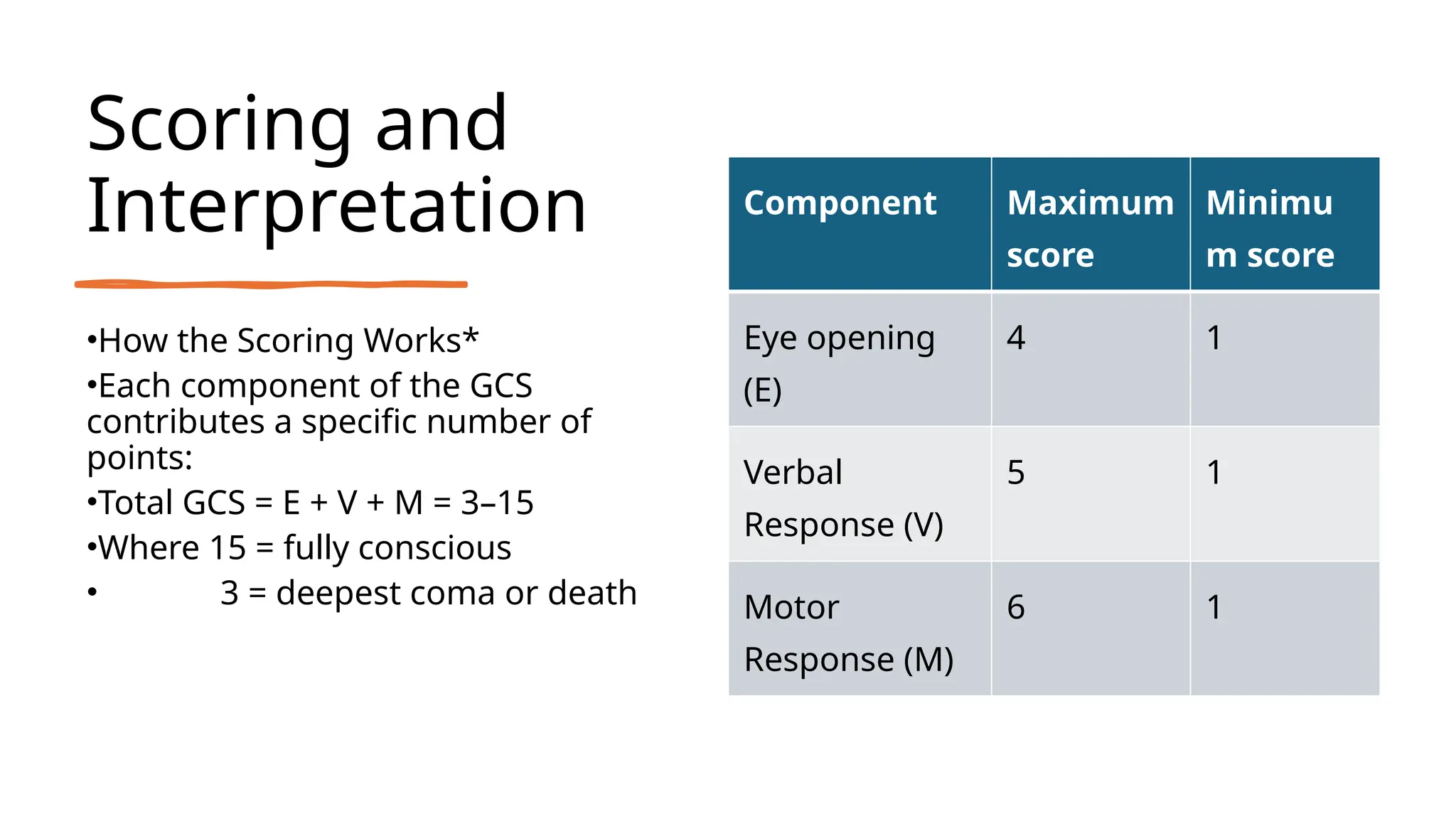
•How theScoring Works*
•Each component of the GCS
contributes a specific number of
points:
•Total GCS = E + V + M = 3–15
•Where 15 = fully conscious
• 3 = deepest coma or death
Component Maximum
score
Minimu
m score
Eye opening
(E)
4 1
Verbal
Response (V)
5 1
Motor
Response (M)
6 1
15.
Interpreting the
Total GCS
•Becausea GCS of 8 or less indicates
inability to protect the airway, and likely
loss of gag and cough reflexes.
•
•Trend is More Important Than One Score
•
• Don’t just write a single GCS score.
• Always compare with previous scores to
see if the patient is improving or
worsening.
Total
score
Level of
Consciousness
Severity Clinical Implications
13-15 Usually
conscious
Mild reassess
9-12 Usually
unconscious
Moderate Risk of deterioration;
admit, monitor ICP
≤8 Usually
unconscious
Severe Airway threatened →
Intubate & ICU
16.
Special Cases
Infants andYoung
Children: Use Modified
Pediatric GCS instead of
verbal speech, note coos,
cries, or irritability. Eye and
motor responses are
interpreted relative to
developmental age.
1
Intubated Patients: Verbal
response can’t be assessed
record as “V – (T)” for
→
tube. Example: “GCS = E3
V(T) M5 = 8T/15.”
2
Sedated or Paralyzed
Patients: Document as
“GCS not assessable –
patient sedated.”
3
17.
LIMITATIONS & CONCLUSION
•Influencedby External Factors: Sedation, alcohol,
drugs, or paralysis can falsely lower scores.
•Intubated or Tracheostomized Patients: Verbal
response can’t be tested must document as “V (T) or
→
not assessable.
•Facial or Eye Injuries: Swelling or trauma can affect
eye-opening assessment.
•Language & Hearing Barriers: Misinterpretation of
commands affects verbal and motor scoring.
•Children & Neonates: Standard GCS not suitable;
requires Modified Pediatric GCS for accurate evaluation.
•Does Not Assess All Neurological Functions: Ignores
pupil reaction, brainstem reflexes, and vital signs — so it
must be used with full neuro exam.