


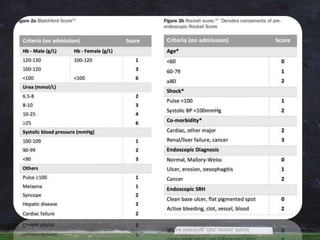
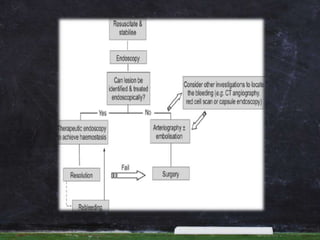



- Acute upper gastrointestinal bleeding is a common medical emergency that can have high mortality. - Risk assessment using tools like the Blatchford and Rockall scores helps determine urgency of endoscopy and predict outcomes. - Endoscopy within 24 hours of admission is recommended to treat bleeding lesions through methods like injection, thermal coagulation, or band ligation of varices. - Post-endoscopic management involves PPIs, transfusions targeting a hemoglobin of 70-90 g/L, H. pylori treatment if present, and continued medications like terlipressin or beta blockers to prevent rebleeding.

































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

