
Recommended
More Related Content
What's hot
What's hot (18)
Similar to German measles (rubella) 2018
Similar to German measles (rubella) 2018 (20)
More from BMCStudents
More from BMCStudents (20)
Recently uploaded
Recently uploaded (20)
German measles (rubella) 2018
- 1. University of Baghdad college of medicine German measles (Rubella) CLS-Pathology Ali Hussein Ahmed Second grade Student selected components 2017/2018
- 2. 2 Contents: 1. Introduction …………………………..……………………………………… 3 2. Search board and discussion: Epidemiology ……………………………………………………………. 4 Signs and symptoms ………………………...…………………………… 6 Causes ……………………………………...…………………………….. 7 Laboratory diagnosis ………………………..…………………………… 7 Vaccine ……………………………………...…………………..……….. 8 Treatment ……………………………………..…………………………. 9 History …………………………………………..…………………..….. 10 Prevention …………………………………………..………………..…. 11 Etymology …………………………………………………………….... 12 3. summary …………………………………………….……………………… 12 4. References …………………………………………….……………………. 13
- 3. 3 INTRODUCTION: Rubella is a directly transmitted immunizing infection that usually occurs during childhood and is associated with low morbidity and mortality. Infection of women during early pregnancy can lead to spontaneous abortion, fetal death or children born with congenital rubella syndrome (CRS), which is associated with multiple disabilities that can require lifelong care [1], including hearing impairment, cataracts and congenital heart disease. [2] A relatively inexpensive, high efficacy vaccine that provides lifelong immunity to rubella and can easily be combined as measles–rubella (MR), or measles–mumps–rubella (MMR) has been available for 50 years. Although routine rubella vaccination can prevent CRS, inadequate vaccination coverage may actually increase CRS cases by increasing the average age of infection [3]; this occurs because vaccination short of the threshold required for elimination effectively reduces incidence in the population, thus reducing the risk of infection and delaying time to the first infection (figure 1). Consequently, introduction of rubella-containing vaccine (RCV) has been limited globally. Recent efforts for the control and elimination of measles have spurred renewed interest in the potential for rubella control, because the two vaccines are easily combined, and overall measles vaccination coverage levels have been climbing [4]. In addition, the Global Alliance for Vaccines Initiative (GAVI) has recently opened a funding window for rubella vaccination [5]. Madagascar is one of the countries that has successfully applied for this funding.
- 4. 4 Fig(1). Theoretical expectations for RCV coverage and the burden of CRS. In a classic SIR framework, the dynamics of susceptibles are captured by dS/dt = μ(1 − v) − βSI − μS; and infected by dI/dt = βSI − gI − μI; where μ is the birth and death rate, total population size as taken as N = 1, v is vaccination coverage of the birth cohort, g is the generation time of the infection and the transmission rate is β = R0(g + μ). To capture rubella dynamics, we set g to 18 days−1, R0 = 5, and chose μ = 30 per 1000 per year. (a) The equilibrium proportion of infected individuals I* (y- axis) is defined by I* = μ[(1 − v)R0 − 1]/β and thus declines with increasing vaccination coverage (x-axis). (b) Conversely, the average age of infection A (y-axis) increases, following R0 = G/A, where G is the inverse of the unvaccinated birth rate, G = 1/[μ(1 − v)]. (c) This conjunction of declining incidence but increasing average age of infection has the potential to yield a situation where more cases are occurring in women of childbearing age, even though the total number of cases is declining. As a result, the ratio of the equilibrium burden of CRS in the presence of vaccination relative to the equilibrium burden of CRS if no vaccination has occurred (y-axis) may first increase with vaccination coverage relative to the scenario of no vaccination (indicated by the horizontal grey line); eventually declining when incidence is sufficiently low to offset the increase in the average age of infection. (Results in the last panel are hypothetical; exact values will depend on the variance and skew of the distribution of age of infection; as well as pattern of fertility over age). This pattern of increasing CRS burden with increasing vaccination coverage has been called ‘the paradoxical increase of rubella’. Epidemiology: Under-reporting in the incidence data affected our ability to estimate the proportion of the population susceptible to rubella (see figure 2a and the electronic supplementary material, S1). However, the TSIR model indicated a clear pattern of seasonality in transmission, with low transmission in February, June and October, which was robust to the range of assumptions about starting proportion susceptible. Surprisingly, the timing of low transmission does not align with summer school holidays, in contrast to what has been reported for rubella and other immunizing childhood infections in many other parts of the world.[6][7][8] Given low reported incidence, we focused our initial descriptive analysis of the epidemiology of rubella in Madagascar at the largest administrative scale available, the six provinces of Madagascar. The average age of infection of rubella is slightly variable across these provinces, ranging from 6.4 years in the province of Antananarivo to 8.8 years in Antsiranana. Average age broadly negatively correlates with province population size (Pearson's correlation between log population size and average age of infection yields ρ = −0.82, n = 6, p < 0.05), suggesting an underlying biological driver for this pattern. Two possible drivers of this average infection age distribution include (i) extinction–recolonization dynamics, which drive up the average age of infection in smaller population provinces [9]—implying that provinces with smaller populations also have
- 5. 5 smaller focal population centres, precluding persistence of rubella or (ii) a higher R0 for rubella in provinces with larger populations (although see [8] for evidence that measles, a similar directly transmitted infections, shows no signature of density-dependent transmission). With the data available, it is not possible to distinguish between these two possibilities. Using the approximation R0 = G/A (which assumes negligible stochastic dynamics), where G is the inverse of the birth rate, and A is the average age of infection, the average age of infection in the data yields estimates of R0 between 3.9 in Antsiranana province and 5.5 in Antananarivo province. This range is broadly in line with values previously reported for this infection.[10][11][12] Fig(2). The epidemiology of rubella in Madagascar. (a) Reported number of cases through time for the entire country; (b) associated estimates of transmission from the TSIR model; (c) age distribution of infection, and average age of infection (vertical lines) associated with each of the six provinces and (d) Map of incidence in regions of Madagascar across the country with colours showing incidence per 1000 inhabitants
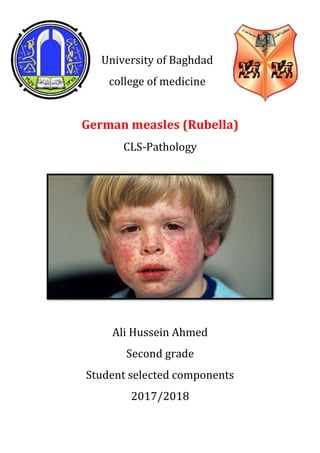
- 6. 6 Signs and symptoms: Rubella has symptoms that are similar to those of flu. However, the primary symptom of rubella virus infection is the appearance of a rash (exanthem) on the face which spreads to the trunk and limbs and usually fades after three days (that is why it is often referred to as three-day measles). The facial rash usually clears as it spreads to other parts of the body. Other symptoms include low grade fever, swollen glands (sub-occipital and posterior cervical lymphadenopathy), joint pains, headache, and conjunctivitis.[13] The swollen glands or lymph nodes can persist for up to a week and the fever rarely rises above 38 °C (100.4 °F). The rash of German measles is typically pink or light red. The rash causes itching and often lasts for about three days. The rash disappears after a few days with no staining or peeling of the skin. When the rash clears up, the skin might shed in very small flakes where the rash covered it. Forchheimer's sign occurs in 20% of cases, and is characterized by small, red papules on the area of the soft palate.[14] Rubella can affect anyone of any age and is generally a mild disease, rare in infants or those over the age of 40. The older the person is the more severe the symptoms are likely to be. Up to 60% of older girls or women experience joint pain or arthritic type symptoms with rubella.[15] In children rubella normally causes symptoms which last two days and include:[16] Rash beginning on the face which spreads to the rest of the body. Low fever of less than 38.3 °C (101 °F.) Posterior cervical lymphadenopathy.[17] In older children and adults additional symptoms may be present including: Swollen glands Coryza (cold-like symptoms) Aching joints (especially in young women) Rare problems can occur including the following: Brain inflammation Fig 3
- 7. 7 Ear infection [18] Coryza in rubella may convert to pneumonia, either direct viral pneumonia or secondary bacterial pneumonia, and bronchitis (either viral bronchitis or secondary bacterial bronchitis).[19] Causes: The disease is caused by rubella virus, a togavirus that is enveloped and has a single-stranded RNA genome.[20] The virus is transmitted by the respiratory route and replicates in the nasopharynx and lymph nodes. The virus is found in the blood 5 to 7 days after infection and spreads throughout the body. The virus has teratogenic properties and is capable of crossing the placenta and infecting the fetus where it stops cells from developing or destroys them.[21] During this incubation period, the patient is contagious typically for about one week before he/she develops a rash and for about one week thereafter. Increased susceptibility to infection might be inherited as there is some indication that HLA-A1 or factors surrounding A1 on extended haplotypes are involved in virus infection or non-resolution of the disease.[22] Laboratory Diagnostics: Clinical specimens for the diagnosis of rubella by virus detection usually consist of throat swabs (TS), oral fluids (OF) or nasopharyngeal secretions, and by antibody detection are usually sera or OF.[23] The virus has also been found in other specimens, including cataract tissue and urine. Urine and TSs or OFs are about equivalent as sources of viral RNA, but the ease of obtaining TSs or OFs make these specimens the primary ones that are collected.[24] Urine is often a source of infectious virus from CRS patients. Specimens for virus detection and for IgM/IgG detection can be transported by standard methods.
- 8. 8 The timing of specimen collection is important in postnatal rubella. Rubella virus-specific IgM is present in sera in only about 50% of rubella cases on the day of rash, but, at five days after rash, most rubella cases have detectable rubella-specific IgM. Most rubella cases are virus positive on the day of rash and may be positive from seven to ten days post rash.[25] Since postnatal rubella is a mild disease of short duration, special effort is required to obtain samples on the day of rash or shortly thereafter. Patients with CRS and congenital rubella infection (CRI) are IgM and virus positive for months; therefore, timing is less critical for individuals suspected of having CRS or CRI.[26] Alternative specimens, such as dried blood spots (DBS) and OF, have recently been shown to be adequate for surveillance of rubella using IgM detection (DBS and OF) and virus detection (OF).[27] Note that diagnostic kits are usually not approved for use with DBS, and low IgM levels in OF necessitate the use of sensitive detection assays. Amplification of rubella virus RNA directly from a clinical specimen using RT- PCR is now common. Assays that can reliably detect 3 to 10 copies of rubella virus RNA are necessary since many specimens have small amounts of rubella RNA. Real-time and nested RT-PCR assays often have this level of sensitivity.[28] Rubella virus specific IgM antibodies are present in people recently infected by rubella virus, but these antibodies can persist for over a year, and a positive test result needs to be interpreted with caution.[29] The presence of these antibodies along with, or a short time after, the characteristic rash confirms the diagnosis.[30] Rubella Vaccine Immunogenetics: The current live rubella virus vaccine strain licensed for use in the United States is the RA27/3 strain. It was first isolated from an infected fetus in the 1960s, and further passaged for attenuation through either the WI-38 or MRC-5 Fig 4
- 9. 9 human diploid cell lines.[31] It is currently administered as a two-dose series in the U.S. as part of the measles-mumps-rubella (MMR-II) vaccine. RA27/3 elicits a robust humoral and cellular immune response. As noted above, correlate protective levels of anti-rubella antibodies are defined as titers at or above 10 IU/ml.70 However, the measurement of rubella-specific humoral immunity using serum antibodies can result in a false positives due to a previous parvovirus or Epstein-Barr virus infection, or the presence of Rh factor.[32] Measuring the response of rubella-specific memory B cells in vaccinees may be an alternative correlate and might explain protective immunity in those individuals with low levels of serum antibodies.81 The seroconversion rate after two doses of MMR-II approaches 99% and antibodies persist for at least 21 years.[33] The high seroconversion rate of 99% is observed as early as 9-months-old after receiving the Wistar RA 27/3 live rubella virus vaccine strain.84 With a calculated half-life of 114 years, rubella-specific antibodies may even persist for an entire lifetime.[34] Although excellent seroconversion rates are obtained with RA27/3 vaccination, there are limited occurrences of vaccine failure, and this is thought to arise when preexisting antibodies neutralize the live viral vaccine strain.[35] Treatment: There is no specific treatment for rubella; however, management is a matter of responding to symptoms to diminish discomfort. Treatment of newborn babies is focused on management of the complications. Congenital heart defectsand cataracts can be corrected by direct surgery.[36] Management for ocular congenital rubella syndrome (CRS) is similar to that for age-related macular degeneration, including counseling, regular monitoring, and the provision of low vision devices, if required.[37] Pregnant women may be treated with antibodies called hyperimmune globulin that can fight off the virus. This can help reduce your symptoms. However, there’s still a chance that your baby will develop congenital rubella syndrome. Babies who are born with congenital rubella will require treatment from a team of specialists. Talk to your doctor if you’re concerned about passing German measles on to your baby.[38]
- 10. 10 History: Rubella was first described in the mid-eighteenth century. Friedrich Hoffmann made the first clinical description of rubella in 1740,which was confirmed by de Bergen in 1752 and Orlow in 1758.[39] In 1814, George de Maton first suggested that it be considered a disease distinct from both measles and scarlet fever. All these physicians were German, and the disease was known as Rötheln (contemporary German Röteln), hence the common name of "German measles".[40] Henry Veale, an English Royal Artillery surgeon, described an outbreak in India. He coined the name "rubella" (from the Latin word, meaning "little red") in 1866.[41] It was formally recognised as an individual entity in 1881, at the International Congress of Medicine in London.[42] In 1914, Alfred Fabian Hess theorised that rubella was caused by a virus, based on work with monkeys.[43] In 1938, Hiro and Tosaka confirmed this by passing the disease to children using filtered nasal washings from acute cases.[44] In 1940, there was a widespread epidemic of rubella in Australia. Subsequently, ophthalmologist Norman McAllister Gregg found 78 cases of congenital cataracts in infants and 68 of them were born to mothers who had caught rubella in early pregnancy.[45] Gregg published an account, Congenital Cataract Following German Measles in the Mother, in 1941. He described a variety of problems now known as congenital rubella syndrome (CRS) and noticed that the earlier the mother was infected, the worse the damage was. Since no vaccine was yet available, some popular magazines promoted the idea of "German measles parties" for infected children to spread the disease to other children (especially girls) to immunize them for life and protect them from later catching the disease when pregnant.[46] The virus was isolated in tissue culture in 1962 by two separate groups led by physicians Parkman and Weller.[47]
- 11. 11 Prevention: Rubella infections are prevented by active immunisation programs using live attenuated virus vaccines. Two live attenuated virus vaccines, RA 27/3 and Cendehill strains, were effective in the prevention of adult disease. However their use in prepubertal females did not produce a significant fall in the overall incidence rate of CRS in the UK. Reductions were only achieved by immunisation of all children.[48] The vaccine is now usually given as part of the MMR vaccine. The WHO recommends the first dose be given at 12 to 18 months of age with a second dose at 36 months. Pregnant women are usually tested for immunity to rubella early on. Women found to be susceptible are not vaccinated until after the baby is born because the vaccine contains live virus.[49] The immunisation program has been quite successful. Cuba declared the disease eliminated in the 1990s, and in 2004 the Centers for Disease Control and Prevention announced that both the congenital and acquired forms of rubella had been eliminated from the United States.[50] Screening for rubella susceptibility by history of vaccination or by serology is recommended in the United States for all women of childbearing age at their first preconception counseling visit to reduce incidence of congenital rubella syndrome (CRS). It is recommended that all susceptible non-pregnant women of childbearing age should be offered rubella vaccination.[51] Due to concerns about possible teratogenicity, use of MMR vaccine is not recommended during pregnancy. Instead, susceptible pregnant women should be vaccinated as soon as possible in the postpartum period.[52]
- 12. 12 Etymology: The name rubella is sometimes confused with rubeola, an alternative name for measles in English-speaking countries; the diseases are unrelated.[53][54] In some other European languages, like Spanish, rubella and rubeola are synonyms, and rubeola is not an alternative name for measles.[55] Thus, in Spanish, "rubeola" refers to rubella and "sarampión" refers to measles. Summary: Rubella remains an important pathogen globally with approximately 100,000 cases of congenital rubella syndrome estimated to occur each year. Rubella vaccine is highly effective and safe when used across a population and, as a result, endemic rubella transmission has been interrupted in the Americas since 2009. Incomplete rubella vaccination programs result in continued disease transmission as evidenced by recent large outbreaks in Japan and elsewhere. Herein, we provide current results regarding rubella control, elimination and eradication policies, and a brief review of new laboratory diagnostics. In addition, we provide novel information regarding rubella vaccine immunogenetics and review the emerging evidence of inter-individual variability in humoral and cell-mediated innate and adaptive immune responses to rubella vaccine and their association with HLA alleles, haplotypes, and single nucleotide polymorphisms across the human genome. Finally, we conclude with a call for further research in rubella vaccine immunogenetics and its ability to inform a vaccinomics-level approach to novel vaccine candidate development and the need for a next generation vaccine that is affordable, easy to administer, and does not require a cold chain for optimal immunogenicity.
- 13. 13 References: 1. Hinman AR, Irons B, Lewis M, Kandola K. 2002. Economic analyses of rubella and rubella vaccines: a global review. Bull. World Health Organ. 80, 264–270. 2. Cooper LZ. 1985. The history and medical consequences of rubella. Rev. Infect. Dis. 7, S2–S10. 3. Knox EG. 1980. Strategy for rubella vaccination. Int. J. Epidemiol. 9, 13–23. 4. Strebel PM, Cochi SL, Hoekstra E, Rota PA, Featherstone D, Bellini WJ, Katz SL. 2011. A world without measles. J. Infect. Dis. 204(Suppl 1), S1–S3. 5. Burki T. 2012. GAVI alliance to roll out rubella vaccine. Lancet Infect. Dis. 6. Metcalf CJE, Bjørnstad ON, Ferrari MJ, Klepac P, Bharti N, Lopez-Gatell H, Grenfell BT. 2011. The epidemiology of rubella in Mexico: seasonality, stochasticity and regional variation. Epidemiol. Infect. 139, 1029–1038. 7. Metcalf CJE, Bjornstad ON, Grenfell BT, Andreasen V. 2009. Seasonality and comparative dynamics of six childhood infections in pre-vaccination Copenhagen. Proc. R. Soc. B 276, 4111–4118. 8. Bjørnstad ON, Finkenstadt B, Grenfell BT. 2002. Endemic and epidemic dynamics of measles: estimating epidemiological scaling with a time series SIR model. Ecol. Monogr. 72, 169–184. 9. Metcalf CJE, Munayco CV, Chowell G, Grenfell BT, Bjornstad ON. 2011. Rubella meta-population dynamics and importance of spatial coupling to the risk of congenital rubella syndrome in Peru. J. R. Soc. Interface 8, 369–376. 10. Lessler J, Metcalf CJE. 2013. Balancing evidence and uncertainty when considering rubella vaccine introduction. PLoS ONE 8, e67639 11. Edmunds WJ, Van De Heijden OG, Eerola M, Gay NJ. 2000. Modelling rubella in Europe. Epidemiol. Infect. 125, 617–634. 12. Cutts FT, Abebe A, Messele T, Dejene A, Enquselassie F, Nigatu W, Nokes DJ. 2000. Sero-epidemiology of rubella in the urban population of Addis Ababa, Ethiopia. Epidemiol. Infect. 124, 467–479. 13. Edlich RF, Winters KL, Long WB, Gubler KD (2005). "Rubella and congenital rubella (German measles)". J Long Term Eff Med Implants. 15 (3): 319–28. 14. Robert Kliegman, Waldo E. Nelson, Hal B. Jenson, Karen J. Marcdante, M.D., Richard E. Behrman. Nelson Essentials of Pediatrics, page 467. Elsevier Health Sciences, 2006.
- 14. 14 15. Robert R. Jarrett. "Numbered Diseases of Childhood: THIRD Disease – Rubella". Pediatric House Calls. Archived from the original on May 17, 2015. Retrieved April 30, 2015. 16. Marissa Selner; Winnie Yu (July 25, 2012). "German Measles (Rubella)". Healthline. 17. Rubella (German Measles)". Archived from the original on 2013-10-06. 18. "Rubella: Complications". Diseases and Conditions. Mayo Foundation for Medical Education and Research. 13 May 2015. Archived from the original on 18 May 2015. 19. Michael, M. (1908). "Rubella: Report of Epidemic of Eighty Cases". In Treat, E.B. Archives of Pediatrics. p. 604. Archived from the original on 2015-11-25. 20. Frey TK (1994). "Molecular biology of rubella virus". Adv. Virus Res. 44: 69– 160. 21. Edlich RF, Winters KL, Long WB, Gubler KD (2005). "Rubella and congenital rubella (German measles)". J Long Term Eff Med Implants. 15 (3): 319–28. 22. Forrest JM, Turnbull FM, Sholler GF, et al. (2002). "Gregg's congenital rubella patients 60 years later". Med. J. Aust. 177 (11–12): 664–7. PMID 12463994. Archived from the original on 2008-08-30. 23. Abernathy E, Cabezas C, Sun H, Zheng Q, Chen MH, Castillo-Solorzano C, et al. Confirmation of rubella within 4 days of rash onset: comparison of rubella virus RNA detection in oral fluid with immunoglobulin M detection in serum or oral fluid. Journal of Clinical Microbiology. 2009;47(1):182–188. 24. Winchester SA, Varga Z, Parmar D, Brown KE. Persistent intraocular rubella infection in a patient with Fuchs' uveitis and congenital rubella syndrome. Journal of Clinical Microbiology. 2013;51(5):1622–1624. 25. Bellini WJ, Icenogle JP. Measles and rubella viruses. In: J V, Carroll KC, Jorgensen JH, Funke G, Landry ML, Warnock DW, editors. Manual of Clinical Microbiology. Washington, D.C: ASM Press; 2011. pp. 1372–1387. 26. Recommendations from an ad hoc Meeting of the WHO Measles and Rubella Laboratory Network (LabNet) on use of alternative diagnostic samples for measles and rubella surveillance. MMWR Morbidity and mortality weekly report. 2008;57(24):657–660.
- 15. 15 27. Jin L, Vyse A, Brown DW. The role of RT-PCR assay of oral fluid for diagnosis and surveillance of measles, mumps and rubella. Bulletin of the World Health Organization. 2002;80(1):76–77. 28. Hubschen JM, Kremer JR, De Landtsheer S, Muller CP. A multiplex TaqMan PCR assay for the detection of measles and rubella virus. Journal of Virological Methods. 2008;149(2):246–250. 29. Best JM (2007). "Rubella". Semin Fetal Neonatal Med. 12 (3): 182–92. 30. Stegmann BJ, Carey JC (2002). "TORCH Infections. Toxoplasmosis, Other (syphilis, varicella-zoster, parvovirus B19), Rubella, Cytomegalovirus (CMV), and Herpes infections". Curr Women's Health Rep. 2 (4): 253–8. 31. Plotkin SA, Farquhar JD, Ogra PL. Immunologic properties of RA27/3 rubella virus vaccine. Journal of the American Medical Association. 1973;225:585–590. 32. Skendzel LP. Rubella immunity. Defining the level of protective antibody. Am J Clin Pathol. 1996;106(2):170–174. 33. Prevention CfDCa. Epidemiology and Prevention of Vaccine-Preventable Diseases. 12th, second printing ed. Washington, D.C: Public Health Foundation; 2012. 34. Kakoulidou M, Ingelman-Sundberg H, Johansson E, Cagigi A, Farouk SE, Nilsson A, et al. Kinetics of antibody and memory B cell responses after MMR immunization in children and young adults. Vaccine. 2013;31(4):711–717. 35. Vaananen P, Makela P, Vaheri A. Effect of low level immunity on response to live rubella virus vaccine. Vaccine. 1986;4(1):5–8 36. Khandekar R, Sudhan A, Jain BK, Shrivastav K, Sachan R (2007). "Pediatric cataract and surgery outcomes in Central India: a hospital based study". Indian J Med Sci. 61 (1): 15–22. doi:10.4103/0019-5359.29593. PMID 17197734. Archived from the original on 2007-10-30. 37. Weisinger HS, Pesudovs K (2002). "Optical complications in congenital rubella syndrome". Optometry. 73 (7): 418–24. 38. inman AR, Irons B, Lewis M, Kandola K. 2002. Economic analyses of rubella and rubella vaccines: a global review. Bull. World Health Organ. 80, 264–270. 39. Wesselhoeft C (1949). "Rubella and congenital deformities". N. Engl. J. Med. 240 (7): 258–61. 40. Best, J.M.; Cooray, S.; Banatvala, J.E. (2005). "45. Rubella". Topley and Wilson's Microbiology and Microbial Infections. 2 Virology. pp. 960–992.
- 16. 16 41. Lee JY, Bowden DS (2000). "Rubella virus replication and links to teratogenicity". Clin. Microbiol. Rev. 13 (4): 571–87. doi:10.1128/CMR.13.4.571- 587.2000. PMC 88950 Freely accessible. PMID 11023958. Archived from the original on 2007-09-05. 42. Smith, J. L. Contributions to the study of Rötheln. Trans. Int. Med. Congr. Phil. 4,14. 1881 43. Hess, Alfred Fabian (1914). "German measles (rubella): an experimental study". Archives of Internal Medicine. Chicago. 13: 913–6. doi:10.1001/archinte.1914.00070120075007. as cited by Enersen, Ole Daniel. "Alfred Fabian Hess". WhoNamedIt. Archived from the original on 2007-09-30. Retrieved 2007-07-03. 44. Atkinson, W; Hamborsky, J; McIntyre, L; Wolfe, S, eds. (2007). "12. Rubella" (PDF). Epidemiology and Prevention of Vaccine-Preventable Diseases (10th ed.). Centers for Disease Control and Prevention. Archived from the original on 2007- 06-20. Retrieved 2007-07-03. 45. Dangerous Pregnancies: Mothers, Disabilities, and Abortion in Modern America Archived 2016-03-04 at the Wayback Machine. Leslie J. Reagan 46. Hess, Alfred Fabian (1914). "German measles (rubella): an experimental study". Archives of Internal Medicine. Chicago. 13: 913–6. doi:10.1001/archinte.1914.00070120075007. as cited by Enersen, Ole Daniel. "Alfred Fabian Hess". WhoNamedIt. Archived from the original on 2007-09-30. Retrieved 2007-07-03. 47. "EPI Newsletter" (PDF). XX (4). Pan American Health Organization. August 1998. Archived (PDF) from the original on 2011-07-19. Retrieved 2007-07-03. 48. Robertson, SE; Cutts, FT; Samuel, R; Diaz-Ortega, JL (1997). "Control of rubella and congenital rubella syndrome (CRS) in developing countries, Part 2: Vaccination against rubella". Bulletin of the World Health Organization. 75 (1): 69–80. 49. Watson JC, Hadler SC, Dykewicz CA, Reef S, Phillips L (1998). "Measles, mumps, and rubella—vaccine use and strategies for elimination of measles, rubella, and congenital rubella syndrome and control of mumps: recommendations of the Advisory Committee on Immunization Practices (ACIP)". MMWR Recomm Rep. 47 (RR-8): 1–57. PMID 9639369. Archived from the original on 2009-09-18.
- 17. 17 50. Dayan GH, Castillo-Solórzano C, Nava M, et al. (2006). "Efforts at rubella elimination in the United States: the impact of hemispheric rubella control". Clin. Infect. Dis. 43 (Suppl 3): S158–63. 51. Centers for Disease Control and Prevention (CDC) (2005). "Elimination of rubella and congenital rubella syndrome—United States, 1969–2004". MMWR Morb. Mortal. Wkly. Rep. 54 (11): 279–82. PMID 15788995. Archived from the original on 2007-10-01. 52. Health Care Guideline: Routine Prenatal Care. Fourteenth Edition. Archived 2012-06-24 at the Wayback Machine. By the Institute for Clinical Systems Improvement July 2010. 53. Merriam-Webster:Rubeola Archived 2009-04-21 at the Wayback Machine. Accessed 2009-09-20. 54. T. E. C. Jr. (January 1972). "Letters to the editor". Pediatrics. 49 (1): 150–1 55. Webster's Online Dictionary: German measles Accessed 2009-09-20