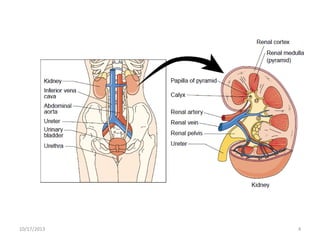
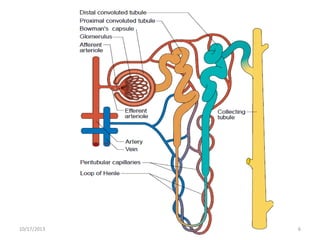
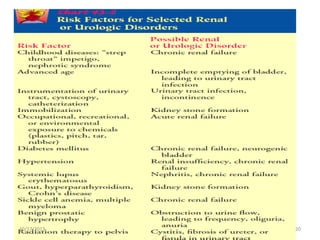
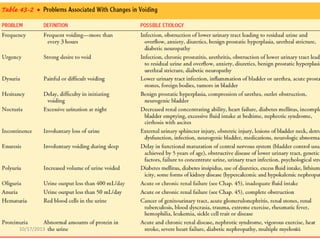
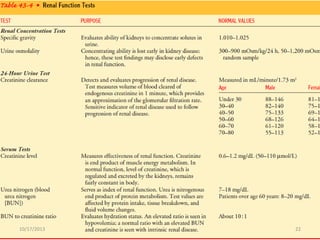
This document provides an overview of genito-urinary disorders and the anatomy and physiology of the urinary system. It describes the key components of the urinary system including the kidneys, ureters, bladder, and urethra. It then focuses on the anatomy and functions of the kidneys, nephrons, glomerulus, and the three step process of urine formation through glomerular filtration, tubular reabsorption, and tubular secretion. Common genito-urinary disorders like urinary tract infections, cystitis, pyelonephritis, prostatitis, urethritis, and nephrotic syndrome are also summarized.






































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


