Downloaded 112 times
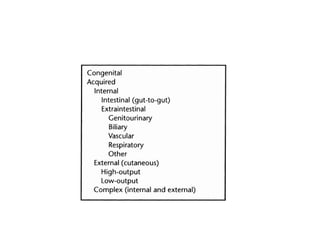

This document summarizes key points about gastrointestinal fistulas: Fistulas are abnormal connections between epithelial surfaces, often between the GI tract and other organs or the skin. GI fistulas can be internal or external. High-output fistulas produce over 500mL/day of output and carry higher risks. Treatment involves recognition, stabilization, investigation to determine the nature and location of the fistula, and definitive treatment such as surgery or medical management.















































