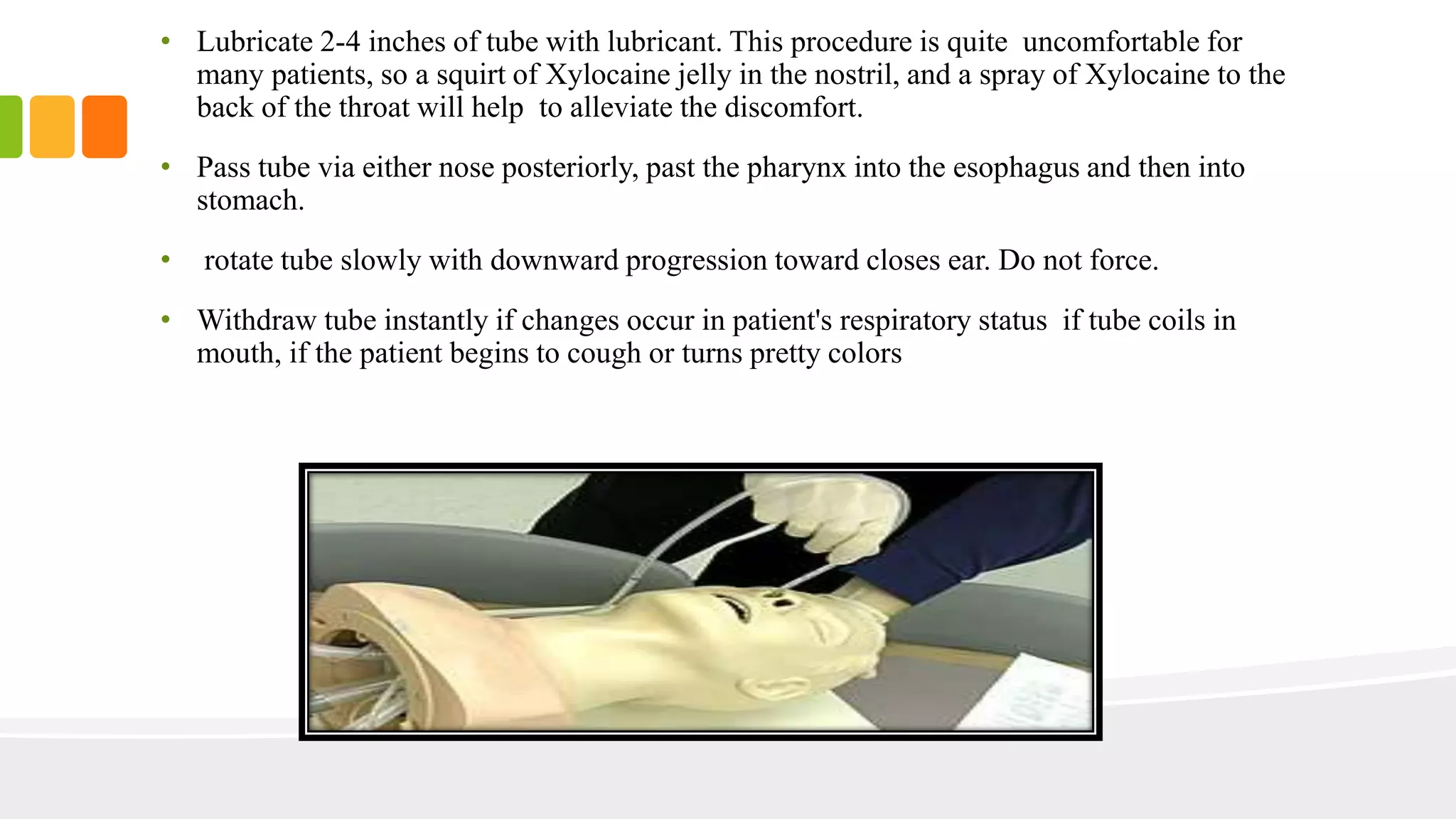
Enteral tube feeding involves inserting a tube into the GI tract to provide nutrition for patients unable to eat normally. Common types are nasogastric tubes inserted through the nose into the stomach and percutaneous endoscopic gastrostomy/jejunostomy tubes inserted through the abdomen into the stomach or jejunum. Proper equipment, positioning, and verification of placement are important to perform these procedures safely. Parenteral nutrition can also be used to provide nutrients intravenously for patients with severe GI issues preventing enteral feeding.