Downloaded 70 times

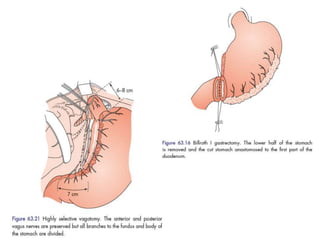
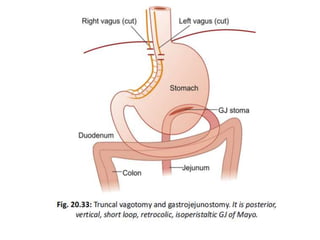


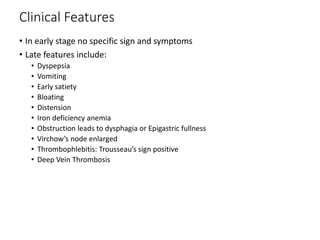
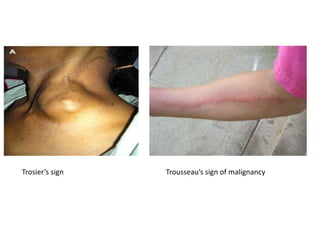



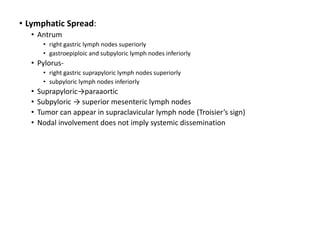

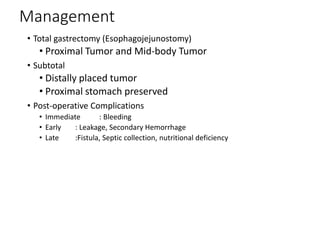


Gastric outlet obstruction has various causes including peptic ulcer disease, gastric cancer, and Crohn's disease. It leads to vomiting of partially digested food, dehydration, and metabolic abnormalities. Diagnosis involves imaging, endoscopy, and biopsy. Management focuses on correcting electrolyte abnormalities and removing the mechanical obstruction endoscopically or surgically via procedures like vagotomy and gastrojejunostomy. Gastric cancer is a common cause and may require total or subtotal gastrectomy depending on location, with postoperative risks of bleeding, leakage, and nutritional deficiencies. Palliative options for inoperable tumors include stenting or bypass procedures.
































![Stomach and duodenum_-_benign_lesions[2]](https://cdn.slidesharecdn.com/ss_thumbnails/stomachandduodenum-benignlesions2-171112093735-thumbnail.jpg?width=640&height=640&fit=bounds)










![STOMACH and DUODENUM SURGERY CLASS[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/stomachandduodenumautosaved-250922162749-cdf69893-thumbnail.jpg?width=640&height=640&fit=bounds)