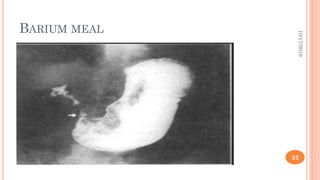
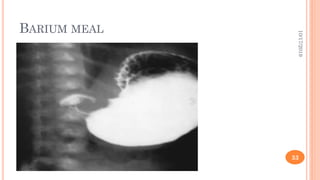
This document provides information on gastric outlet obstruction (GOO), including its definition, causes, pathophysiology, clinical presentation, investigations, and management. It presents the case of a 59-year-old male patient who presented with generalized weakness, postprandial vomiting, and weight loss. Endoscopic biopsy revealed gastric carcinoma known as linitis plastica, resulting in a diagnosis of GOO secondary to gastric malignancy. The document discusses benign and malignant causes of GOO, and the metabolic effects, clinical features, and approach to investigating and initially managing a patient with GOO.






















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




