Downloaded 54 times









![Computer-controlled Local Anesthetic
Delivery Systems [CCLAD]
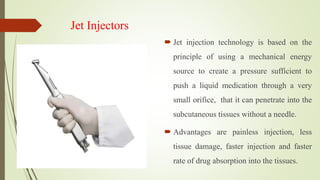
It is essential to deliver local
anesthetic solution at a
constant rate and slower
speed to avoid causing
discomfort to the patient.](https://image.slidesharecdn.com/painandperiodontics-191123041124/85/Pain-and-periodontics-85-320.jpg)

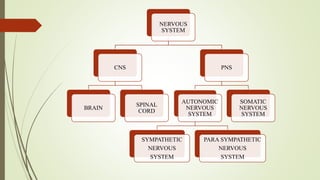
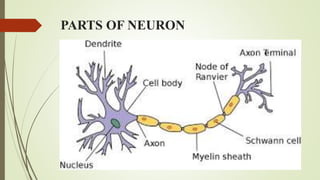
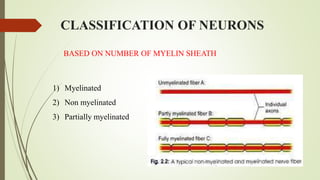
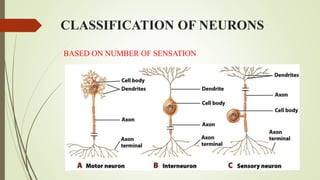
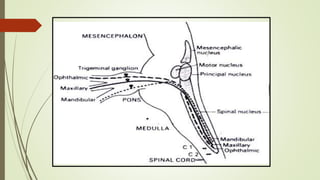
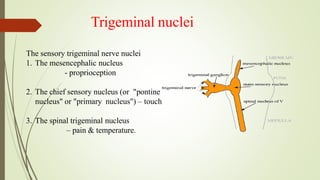
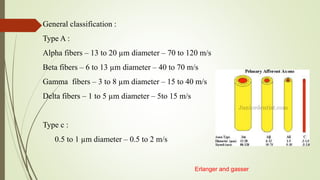
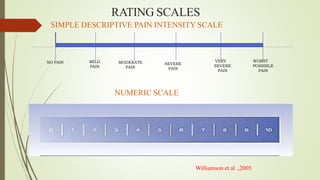
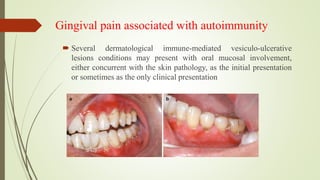
This document provides information about pain and its relation to periodontics. It begins with definitions of pain, including the International Association for the Study of Pain's definition. It then discusses the historical understanding of pain, classifications of pain, and theories of pain mechanisms. The document outlines the nervous system components involved in pain perception and pathways. It discusses assessment of pain and specific types of periodontal and gingival pain, including their characteristics and diagnostic criteria. Overall, the document provides a comprehensive overview of the physiology and experience of pain as it relates to periodontal conditions and treatments.
































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









