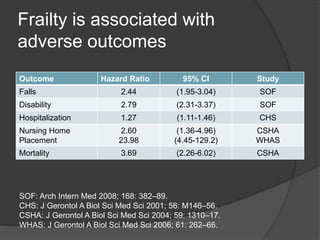
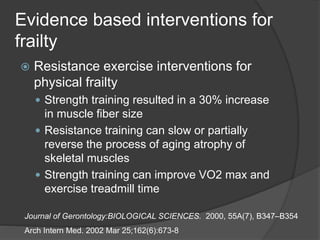
Frailty is a state of increased vulnerability resulting from cumulative decline across multiple physiological systems, leaving the elderly vulnerable to minor stressors that could significantly deteriorate their health. It is common, affecting 15% of non-institutionalized elders, and associated with adverse outcomes like falls, disability, nursing home placement and mortality. While frailty was traditionally viewed as an inevitable part of aging, evidence shows that resistance exercise and nutrition interventions can potentially prevent or partially reverse frailty's declines in muscle mass, strength, and physical performance. Emerging technologies also offer promising tools to address frailty's physical, cognitive and social dimensions but require further assessment and adaptation for elderly users.