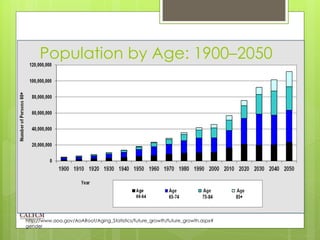
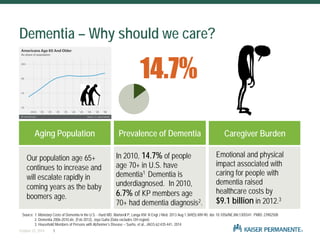
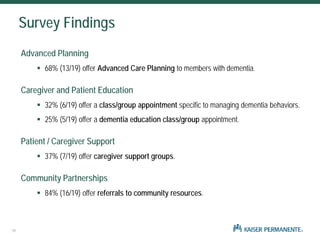
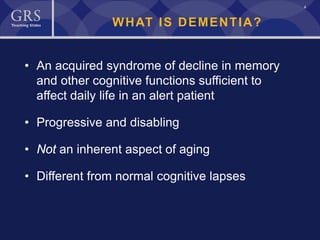
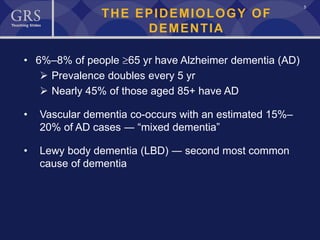
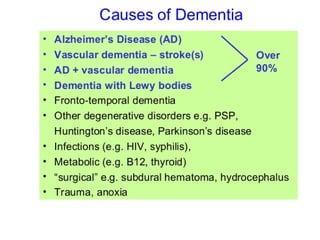
The document outlines the significance of dementia, detailing its prevalence, risk factors, and the societal impact as the aging population grows. It provides a comprehensive overview of assessment methods, differential diagnoses, treatment options, and community resources for managing dementia. Additionally, it highlights the importance of advance care planning and non-pharmacologic interventions in improving the quality of life for patients and caregivers.