Downloaded 1,258 times
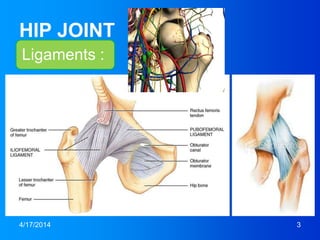
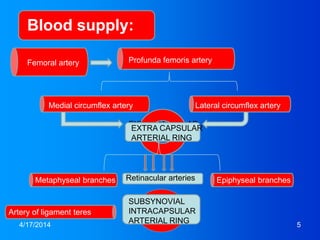
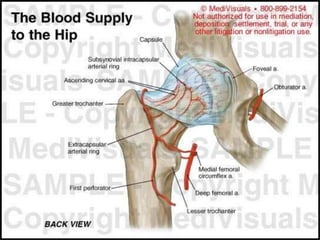
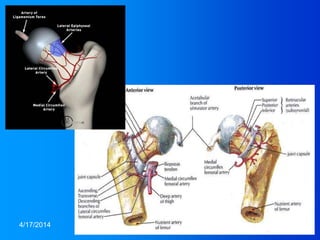
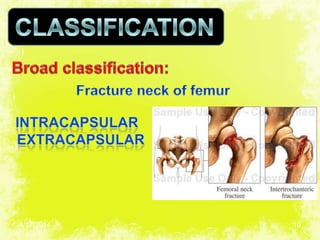
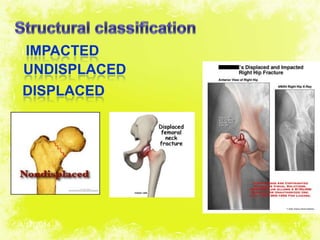

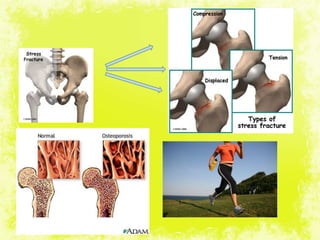
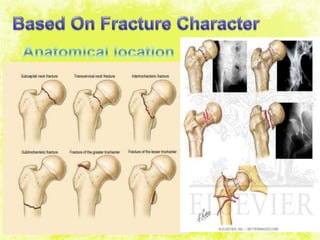
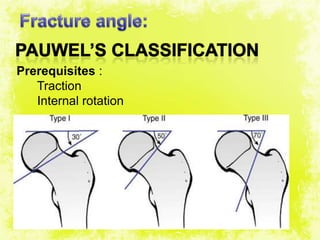
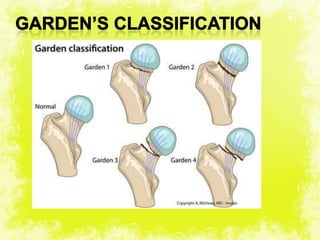
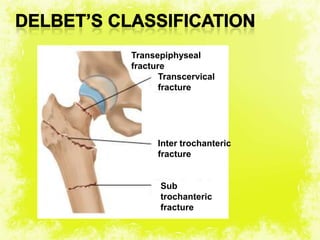
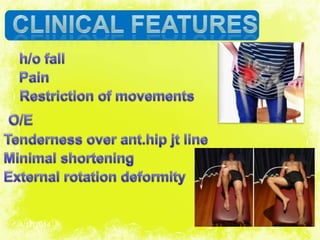

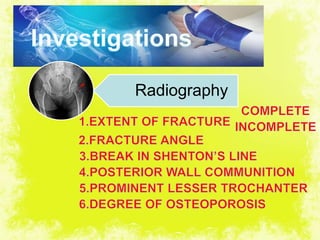
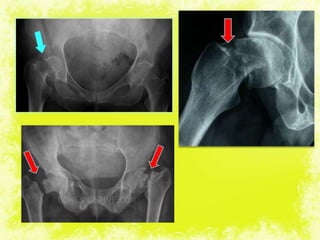
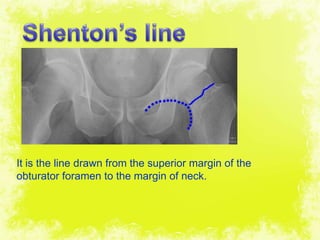
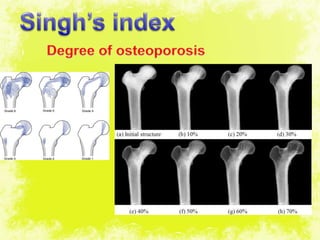

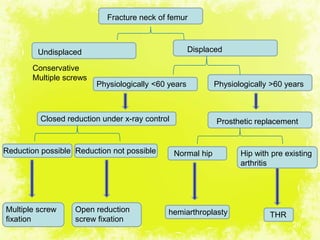
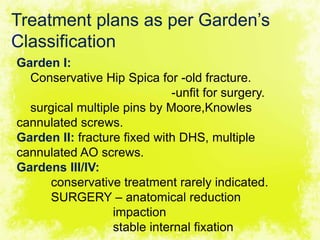


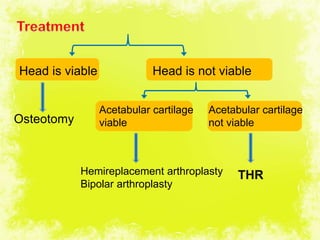

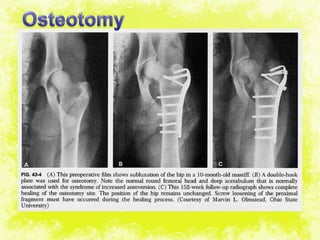
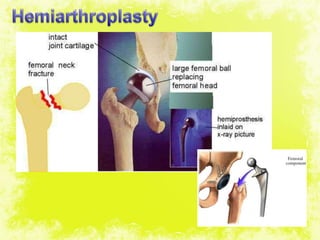
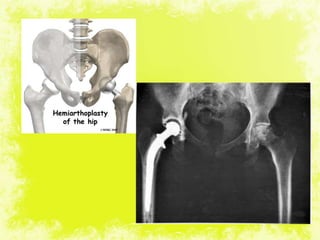
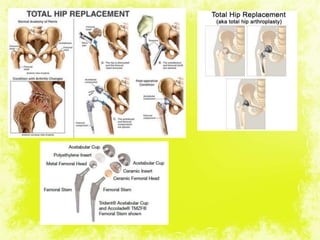
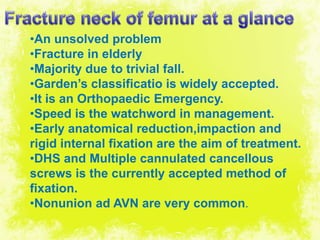


This document discusses the anatomy, causes, classification, symptoms, diagnosis, and treatment of hip fractures. It focuses on fractures of the femoral neck. The hip joint is supported by ligaments and supplied by arteries. Femoral neck fractures most commonly occur in older patients due to falls and osteoporosis. They are classified based on displacement and stability. Treatment depends on the fracture type and patient age or health, and may involve closed or open reduction, internal fixation with screws or plates, or replacement arthroplasty. Complications can include nonunion, avascular necrosis, and failure of internal fixation.






























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)




